

Distinguishing active pediatric COVID-19 pneumonia from MIS-C
- PMID: 33627147
- PMCID: PMC7903373
- DOI: 10.1186/s12969-021-00508-2
Distinguishing active pediatric COVID-19 pneumonia from MIS-C
Abstract
Importance: Active pediatric COVID-19 pneumonia and MIS-C are two disease processes requiring rapid diagnosis and different treatment protocols.
Objective: To distinguish active pediatric COVID-19 pneumonia and MIS-C using presenting signs and symptoms, patient characteristics, and laboratory values.
Design: Patients diagnosed and hospitalized with active COVID-19 pneumonia or MIS-C at Children's of Alabama Hospital in Birmingham, AL from April 1 through September 1, 2020 were identified retrospectively. Active COVID-19 and MIS-C cases were defined using diagnostic codes and verified for accuracy using current US Centers for Disease Control case definitions. All clinical notes were reviewed for documentation of COVID-19 pneumonia or MIS-C, and clinical notes and electronic medical records were reviewed for patient demographics, presenting signs and symptoms, prior exposure to or testing for the SARS-CoV-2 virus, laboratory data, imaging, treatment modalities and response to treatment.
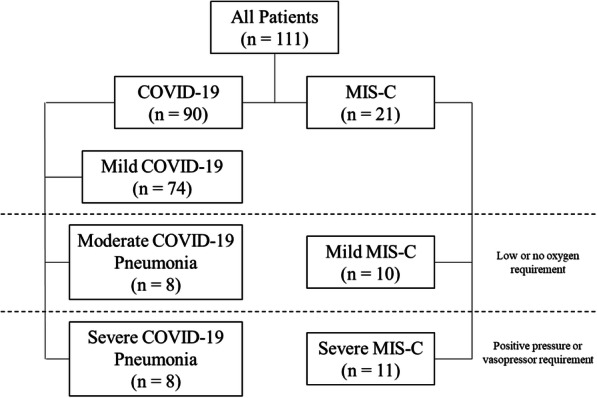
Findings: 111 patients were identified, with 74 classified as mild COVID-19, 8 patients as moderate COVID-19, 8 patients as severe COVID-19, 10 as mild MIS-C and 11 as severe MIS-C. All groups had a male predominance, with Black and Hispanic patients overrepresented as compared to the demographics of Alabama. Most MIS-C patients were healthy at baseline, with most COVID-19 patients having at least one underlying illness. Fever, rash, conjunctivitis, and gastrointestinal symptoms were predominant in the MIS-C population whereas COVID-19 patients presented with predominantly respiratory symptoms. The two groups were similar in duration of symptomatic prodrome and exposure history to the SARS-CoV-2 virus, but MIS-C patients had a longer duration between presentation and exposure history. COVID-19 patients were more likely to have a positive SAR-CoV-2 PCR and to require respiratory support on admission. MIS-C patients had lower sodium levels, higher levels of C-reactive protein, erythrocyte sedimentation rate, d-dimer and procalcitonin. COVID-19 patients had higher lactate dehydrogenase levels on admission. MIS-C patients had coronary artery changes on echocardiography more often than COVID-19 patients.
Conclusions and relevance: This study is one of the first to directly compare COVID-19 and MIS-C in the pediatric population. The significant differences found between symptoms at presentation, demographics, and laboratory findings will aide health-care providers in distinguishing the two disease entities.
Conflict of interest statement
Dr. Reiff has nothing to disclose.
Dr. Samuy has nothing to disclose.
Dr. Scalici reports grants from PCORI, outside the submitted work.
Dr. Mannion has nothing to disclose.
Dr. Cron reports other from Pfizer, personal fees from Novartis, grants and personal fees from SOBI, outside the submitted work.
References
-
- CDC COVID Data Tracker. Centers for Disease Control and Prevention Web Site. https://covid.cdc.gov/covid-data-tracker/#trends_dailytrends. .
-
- Alabama’s COVID-19 Data and Surveillance Dashboard. Alabama Public Health Web Site. https://alpublichealth.maps.arcgis.com/apps/opsdashboard/index.html#. Accessed September 24, 2020.
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
