

Mechanism and reversal of drug-induced nephrotoxicity on a chip
- PMID: 33627489
- PMCID: PMC8897043
- DOI: 10.1126/scitranslmed.abd6299
Mechanism and reversal of drug-induced nephrotoxicity on a chip
Abstract
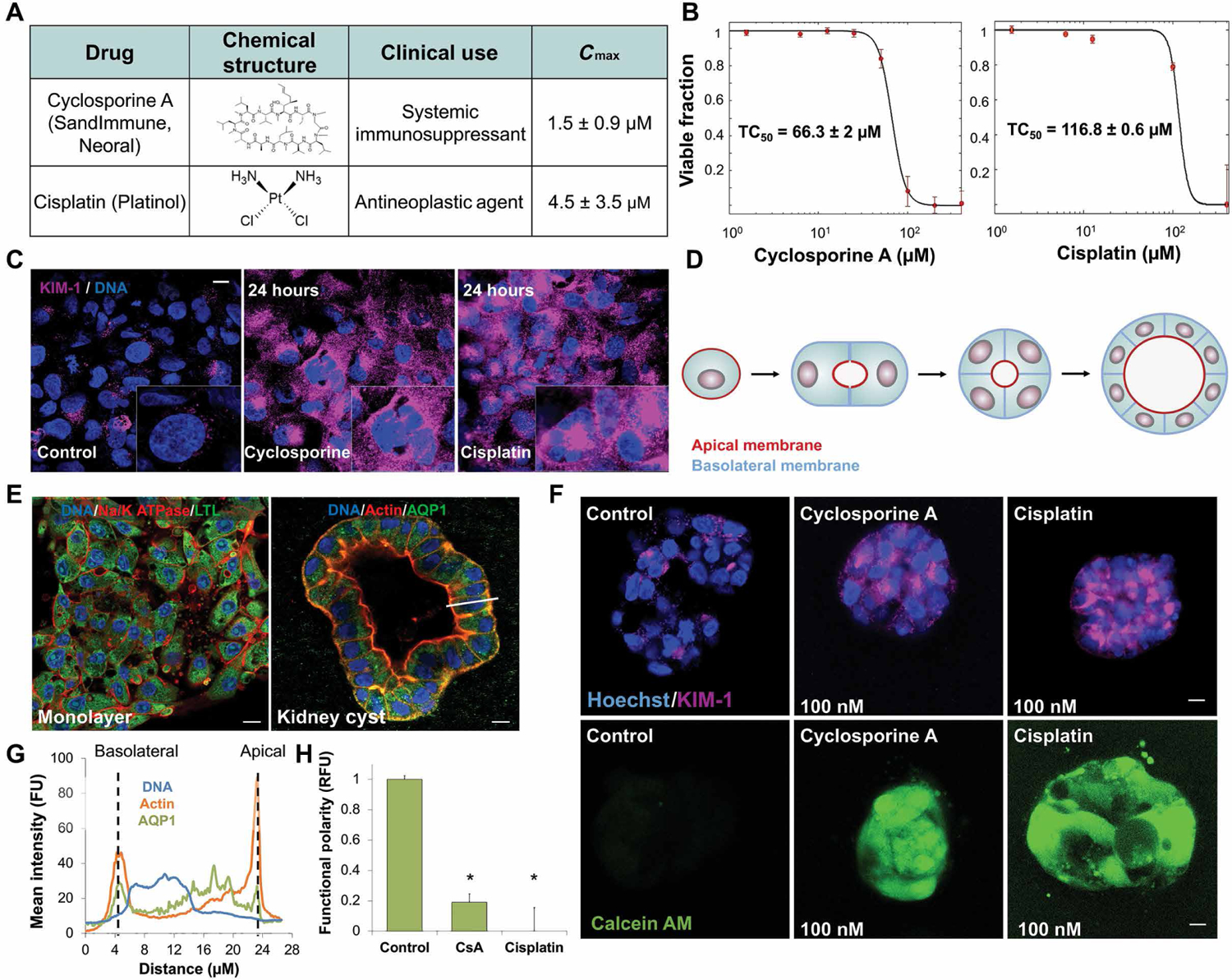
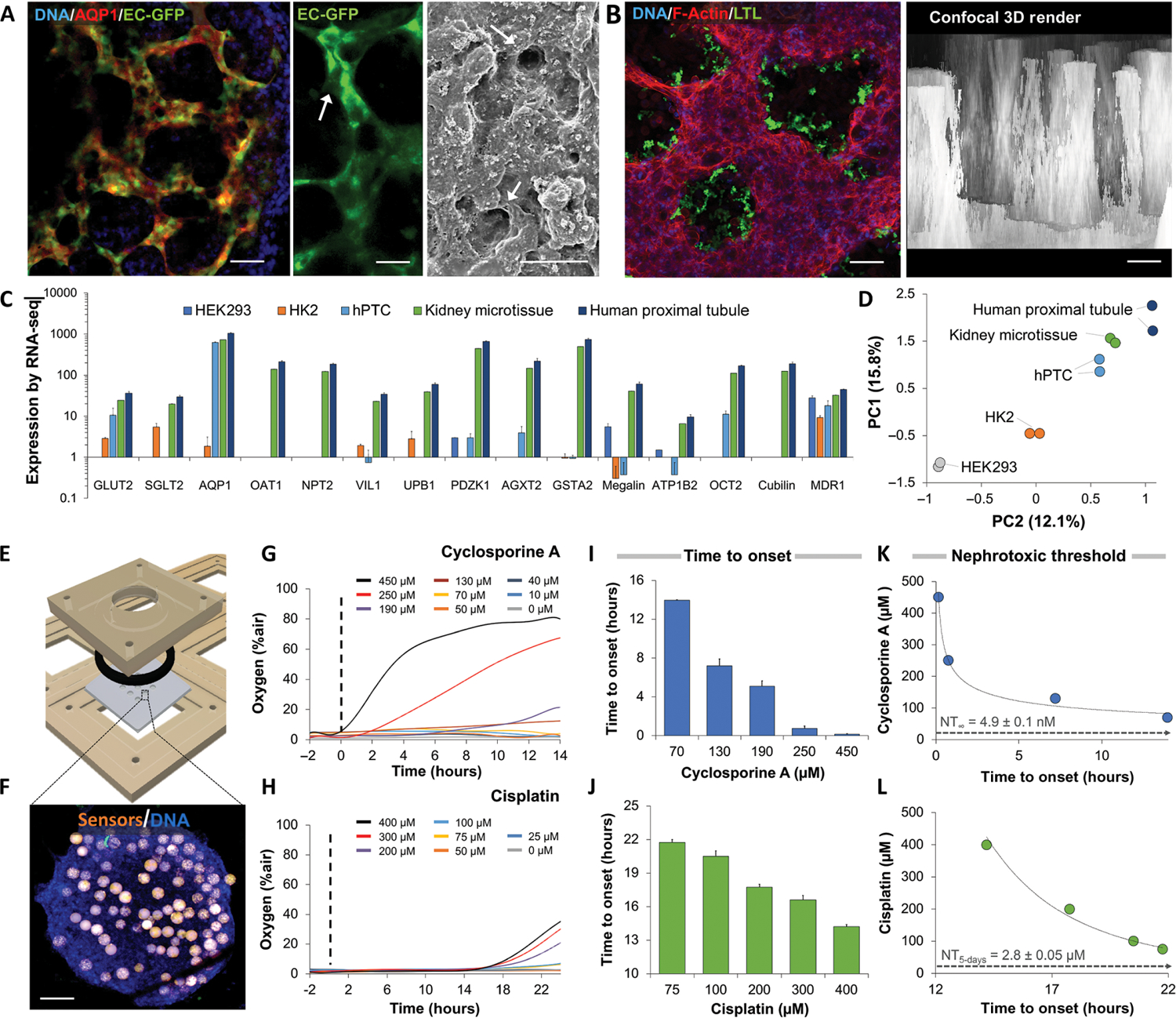
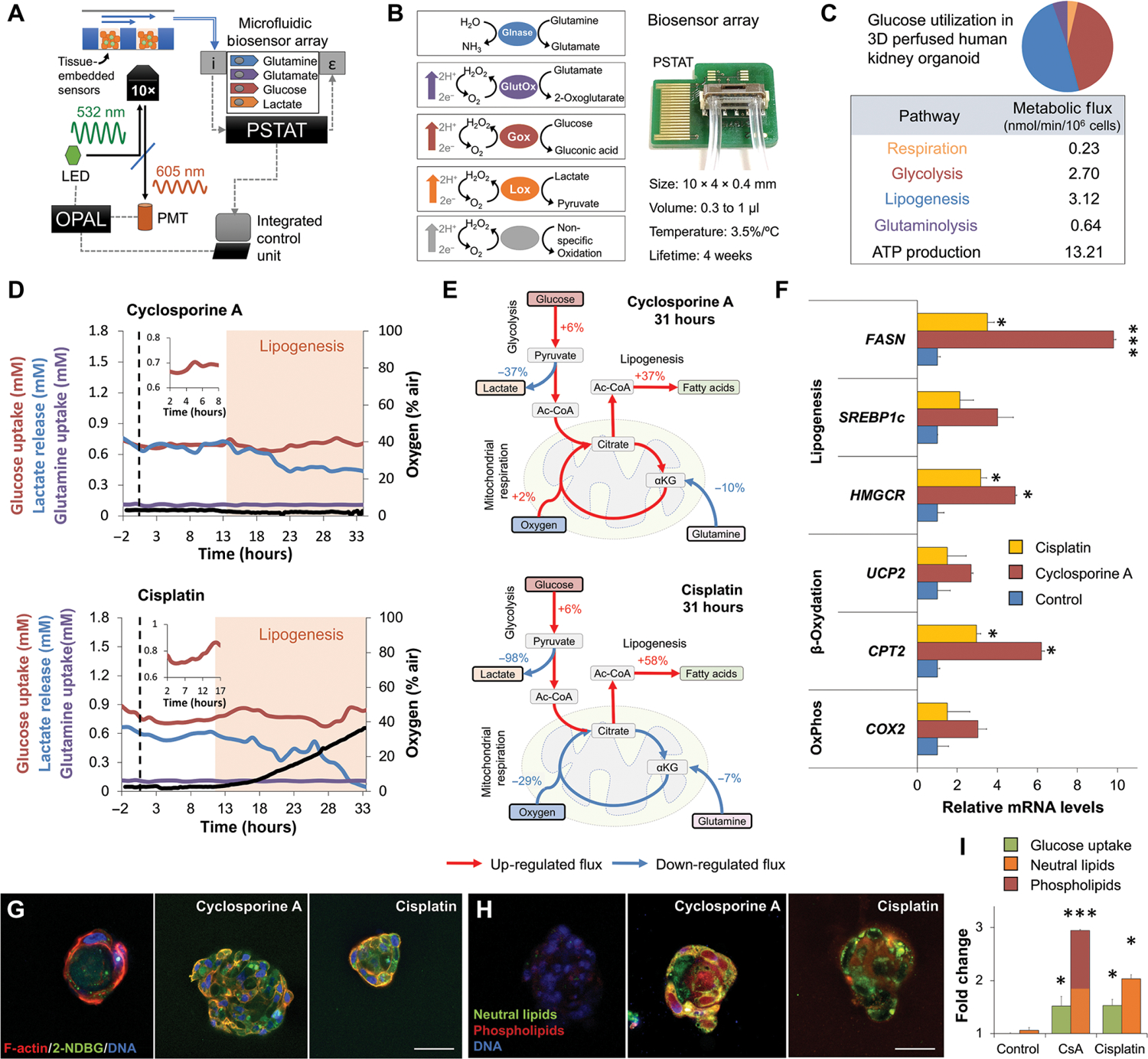
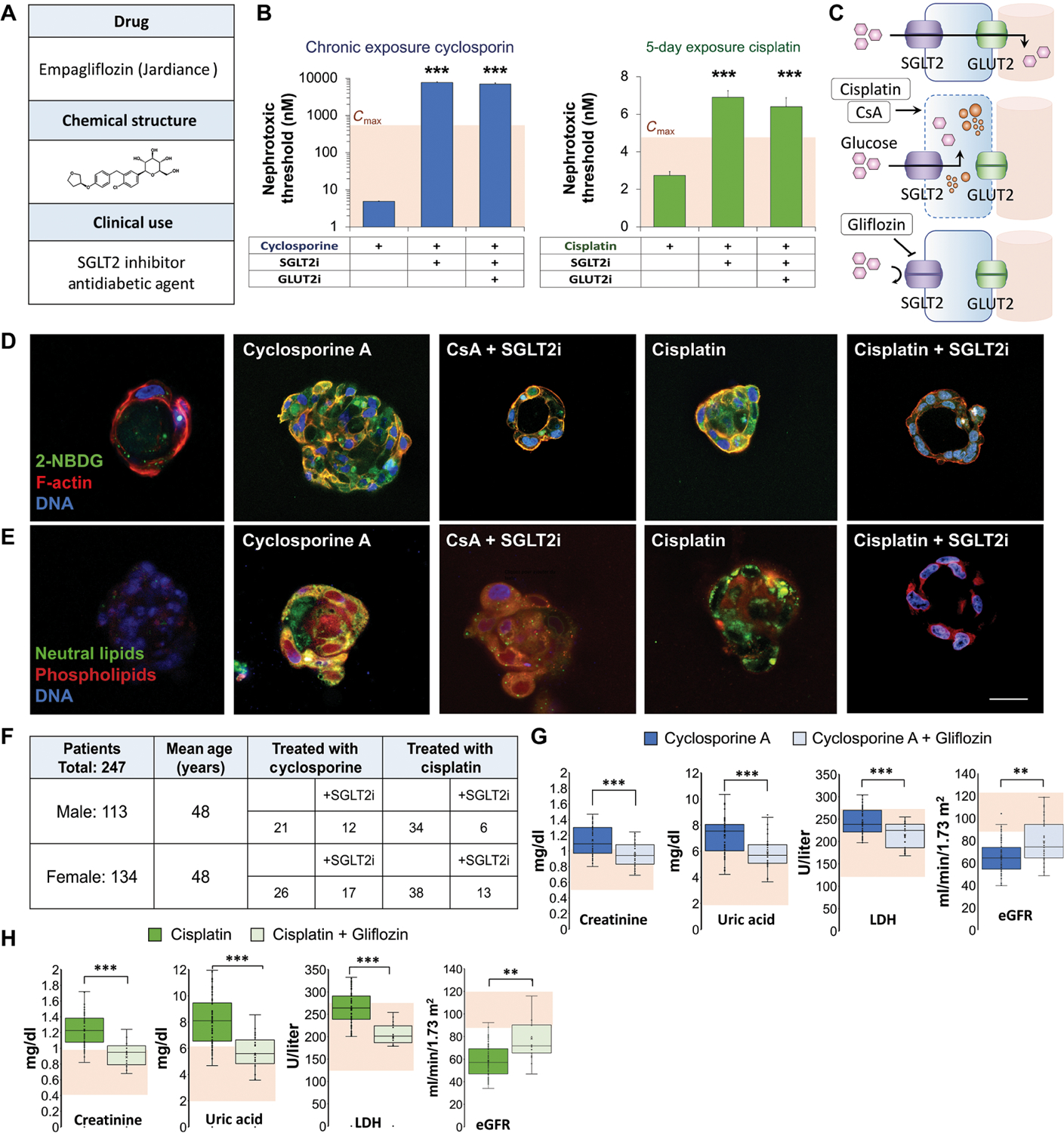
The kidney plays a critical role in fluid homeostasis, glucose control, and drug excretion. Loss of kidney function due to drug-induced nephrotoxicity affects over 20% of the adult population. The kidney proximal tubule is a complex vascularized structure that is particularly vulnerable to drug-induced nephrotoxicity. Here, we introduce a model of vascularized human kidney spheroids with integrated tissue-embedded microsensors for oxygen, glucose, lactate, and glutamine, providing real-time assessment of cellular metabolism. Our model shows that both the immunosuppressive drug cyclosporine and the anticancer drug cisplatin disrupt proximal tubule polarity at subtoxic concentrations, leading to glucose accumulation and lipotoxicity. Impeding glucose reabsorption using glucose transport inhibitors blocked cyclosporine and cisplatin toxicity by 1000- to 3-fold, respectively. Retrospective study of 247 patients who were diagnosed with kidney damage receiving cyclosporine or cisplatin in combination with the sodium-glucose cotransporter-2 (SGLT2) inhibitor empagliflozin showed significant (P < 0.001) improvement of kidney function, as well as reduction in creatinine and uric acid, markers of kidney damage. These results demonstrate the potential of sensor-integrated kidney-on-chip platforms to elucidate mechanisms of action and rapidly reformulate effective therapeutic solutions, increasing drug safety and reducing the cost of clinical and commercial failures.
Copyright © 2021 The Authors, some rights reserved; exclusive licensee American Association for the Advancement of Science. No claim to original U.S. Government Works.
Conflict of interest statement
Figures
Comment in
-
Blocking glucose to reduce drug-induced lipotoxicity.Nat Rev Nephrol. 2021 May;17(5):297. doi: 10.1038/s41581-021-00416-4. Nat Rev Nephrol. 2021. PMID: 33731865 No abstract available.
References
-
- Schetz M, Dasta J, Goldstein S, Golper T, Drug-induced acute kidney injury. Curr. Opin. Crit. Care 11, 555–565 (2005). - PubMed
-
- Perazella MA, Crystal-induced acute renal failure. Am. J. Med 106, 459–465 (1999). - PubMed
-
- Pisoni R, Ruggenenti P, Remuzzi G, Drug-induced thrombotic microangiopathy: Incidence, prevention and management. Drug Saf. 24, 491–501 (2001). - PubMed
-
- Medina PJ, Sipols JM, George JN, Drug-associated thrombotic thrombocytopenic purpura-hemolytic uremic syndrome. Curr. Opin. Hematol 8, 286–293 (2001). - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
