

Cannabis use and cannabis use disorder
- PMID: 33627670
- PMCID: PMC8655458
- DOI: 10.1038/s41572-021-00247-4
Cannabis use and cannabis use disorder
Abstract
Cannabis use disorder (CUD) is an underappreciated risk of using cannabis that affects ~10% of the 193 million cannabis users worldwide. The individual and public health burdens are less than those of other forms of drug use, but CUD accounts for a substantial proportion of persons seeking treatment for drug use disorders owing to the high global prevalence of cannabis use. Cognitive behavioural therapy, motivational enhancement therapy and contingency management can substantially reduce cannabis use and cannabis-related problems, but enduring abstinence is not a common outcome. No pharmacotherapies have been approved for cannabis use or CUD, although a number of drug classes (such as cannabinoid agonists) have shown promise and require more rigorous evaluation. Treatment of cannabis use and CUD is often complicated by comorbid mental health and other substance use disorders. The legalization of non-medical cannabis use in some high-income countries may increase the prevalence of CUD by making more potent cannabis products more readily available at a lower price. States that legalize medical and non-medical cannabis use should inform users about the risks of CUD and provide information on how to obtain assistance if they develop cannabis-related mental and/or physical health problems.
Figures
References
-
-
United Nations. World Drug Report 2020 (2020).
This work provides the most recent global estimates of the prevalence of cannabis use.
-
-
- Peacock A et al. Global statistics on alcohol, tobacco and illicit drug use: 2017 status report. Addiction 113, 1905–1926 (2018). - PubMed
-
- Carvalho AF et al. Cannabis use and suicide attempts among 86,254 adolescents aged 12–15 years from 21 low- and middle-income countries. Eur. Psychiatry 56, 8–13 (2019). - PubMed
-
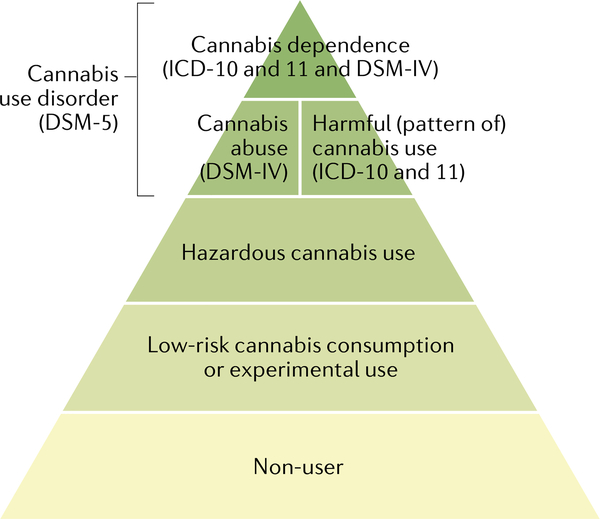
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders: DSM-5 (American Psychiatric Association, 2013).
-
- World Health Organization. International Classification of Diseases for Mortality and Morbidity Statistics (11th Revision) (WHO, version 09/2020). https://icd.who.int/browse11/l-m/en
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
