

Posttraumatic Arachnoid Cyst in the Thoracic Spine with Medullary Compression: Case Report
- PMID: 33627910
- PMCID: PMC7895629
- DOI: 10.1055/s-0040-1714225
Posttraumatic Arachnoid Cyst in the Thoracic Spine with Medullary Compression: Case Report
Abstract
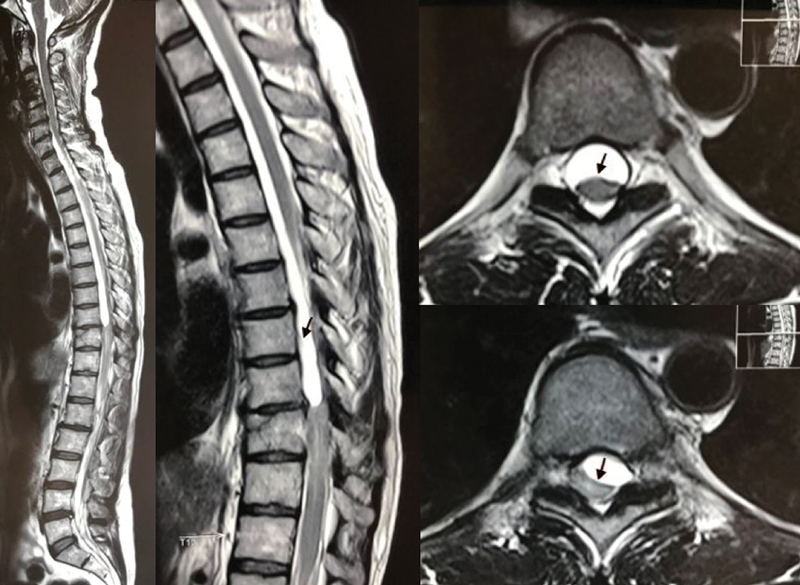
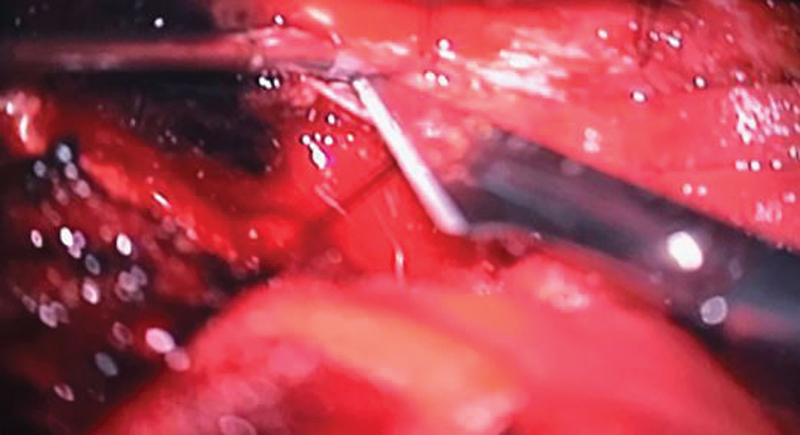
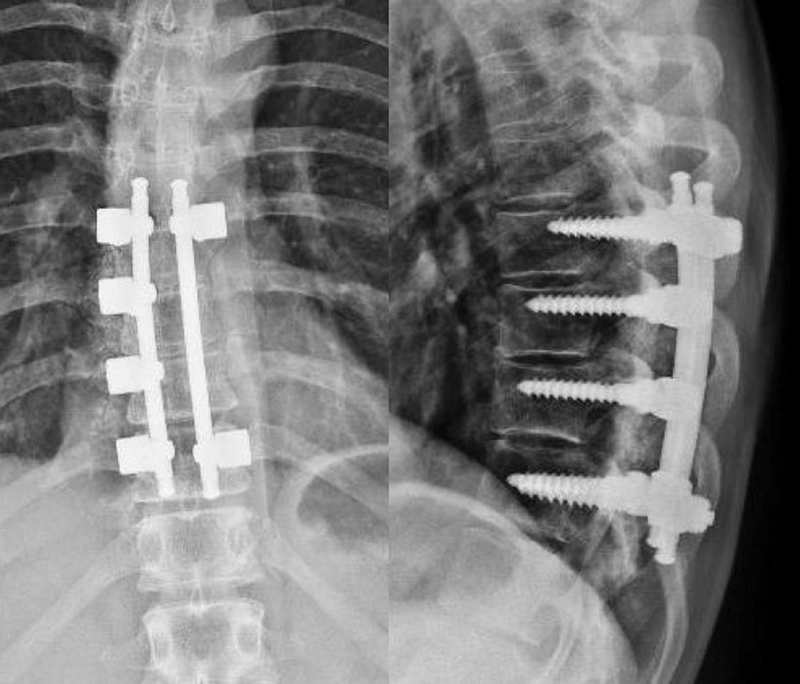
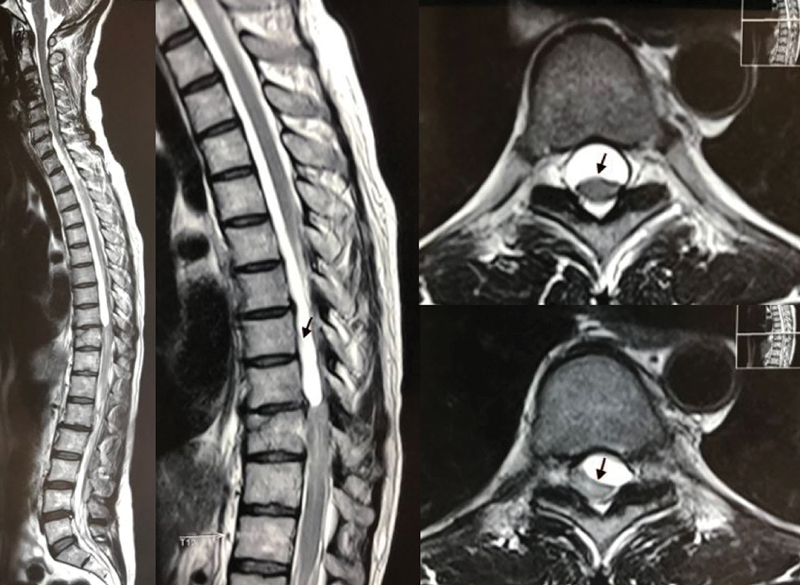
Arachnoid cysts are rare; they can occur at all levels of the dural sac, and can have a congenital, traumatic, iatrogenic or inflammatory origin. In the present article, we report a patient presenting a compressive thoracic myelopathy due to an unusual intradural arachnoid cyst with posttraumatic manifestation and its resolution, in addition to a literature review on the subject. These cysts mainly occur at the thoracic spine, followed by the lumbar, lumbosacral and thoracolumbar spines. Traumatic cysts are caused by an injury to the inner dural layer. These lesions produce neurological deficits through a mass effect on the spinal cord. Concomitant compressive myelopathy is even rarer. In case of myelopathy, cyst resection or drainage is the treatment of choice, and it must be performed immediately. Although rare, arachnoid cysts can be a complication of spine fractures; as such, orthopedists and neurosurgeons, who commonly see these injuries, must be prepared for this unusual situation.
Keywords: arachnoid cysts; spinal cord compression; spinal cord injuries.
Sociedade Brasileira de Ortopedia e Traumatologia. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. ( https://creativecommons.org/licenses/by-nc-nd/4.0/ ).
Conflict of interest statement
Conflitos de Interesses Os autores declaram não haver conflito de interesses.
Figures






Similar articles
-
Review/Perspective On the Diagnosis and Surgical Management of Spinal Arachnoid Cysts.Surg Neurol Int. 2022 Mar 25;13:98. doi: 10.25259/SNI_153_2022. eCollection 2022. Surg Neurol Int. 2022. PMID: 35399888 Free PMC article. Review.
-
Intradural Spinal Arachnoid Cyst: A Long-Term Postlaminectomy Complication: A Case Report and Review of the Literature.World Neurosurg. 2016 Jan;85:367.e1-4. doi: 10.1016/j.wneu.2015.09.058. Epub 2015 Sep 30. World Neurosurg. 2016. PMID: 26428320 Review.
-
Spinal intradural arachnoid cysts located anterior to the cervical spinal cord. Report of two cases and review of the literature.J Neurosurg. 1999 Oct;91(2 Suppl):211-5. doi: 10.3171/spi.1999.91.2.0211. J Neurosurg. 1999. PMID: 10505507 Review.
-
Noncommunicating spinal extradural arachnoid cyst causing spinal cord compression in a child.J Neurosurg. 2005 Sep;103(3 Suppl):266-9. doi: 10.3171/ped.2005.103.3.0266. J Neurosurg. 2005. PMID: 16238081
-
Spinal intradural extramedullary arachnoid cysts in adults-operative therapy and clinical outcome.Acta Neurochir (Wien). 2020 Mar;162(3):691-702. doi: 10.1007/s00701-019-04156-0. Epub 2019 Dec 7. Acta Neurochir (Wien). 2020. PMID: 31813001
Cited by
-
Review/Perspective On the Diagnosis and Surgical Management of Spinal Arachnoid Cysts.Surg Neurol Int. 2022 Mar 25;13:98. doi: 10.25259/SNI_153_2022. eCollection 2022. Surg Neurol Int. 2022. PMID: 35399888 Free PMC article. Review.
References
-
- Shibata T, Nakamura H, Yamano Y. Intradural arachnoid cyst associated with thoracic spinal compression fracture: 7-year follow up after surgery. Spinal Cord. 2001;39(11):599–601. - PubMed
-
- Hernández-León O, Pérez-Nogueira F R, Corrales N. [Postraumatic epidural arachnoid spinal cyst: case report] Neurocirugia (Astur) 2011;22(03):267–270. - PubMed
-
- Vaccaro A R, Oner C, Kepler C K. AOSpine thoracolumbar spine injury classification system: fracture description, neurological status, and key modifiers. Spine. 2013;38(23):2028–2037. - PubMed
-
- Chen H J, Chen L. Traumatic interdural arachnoid cyst in the upper cervical spine. Case report. J Neurosurg. 1996;85(02):351–353. - PubMed
LinkOut - more resources
Full Text Sources