

Safe Gynecological Laparoscopic Surgery during COVID Times
- PMID: 33627981
- PMCID: PMC7879845
- DOI: 10.4103/jhrs.JHRS_185_20
Safe Gynecological Laparoscopic Surgery during COVID Times
Abstract
Background: SARS-CoV-2 virus is largely transmitted via respiratory droplets and the highest transmission risks arise when undertaking aerosol generating procedures like laparoscopy. Most national societies had advised the urgent suspension of elective surgery with the focus shifting to emergency and cancer surgery only during this pandemic. However very little is known regarding the risks to the health care professionals undertaking emergency laparoscopic procedures.
Aims and objective: To demonstrate safety at laparoscopy by modifying the technique for safe management of patients during the COVID-19 pandemic.
Design and setting: This is an observational cohort study. This study was done at a tertiary care reference hospital for minimal access gynaecological surgery. Safety of 42 semi-urgent and emergency laparoscopic surgeries in patients was evaluated for a period of 5 months after taking informed written consent of patients to participate in the study.
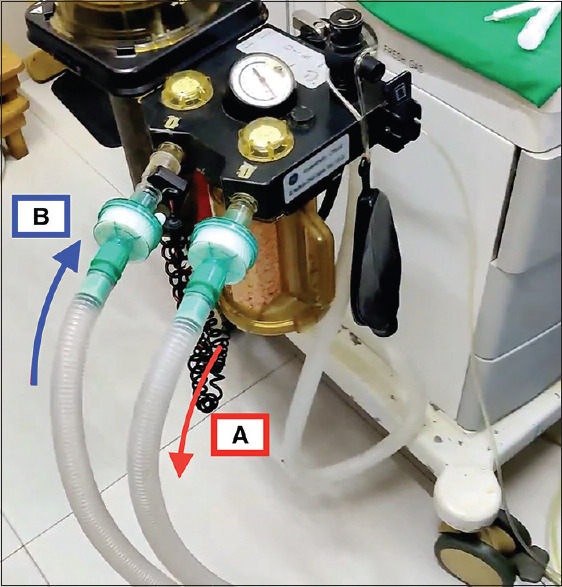
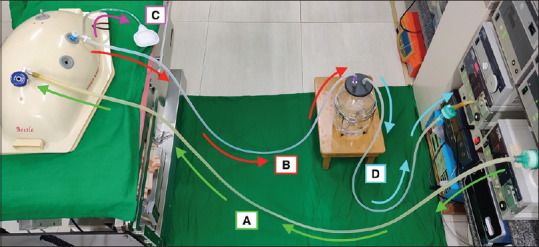
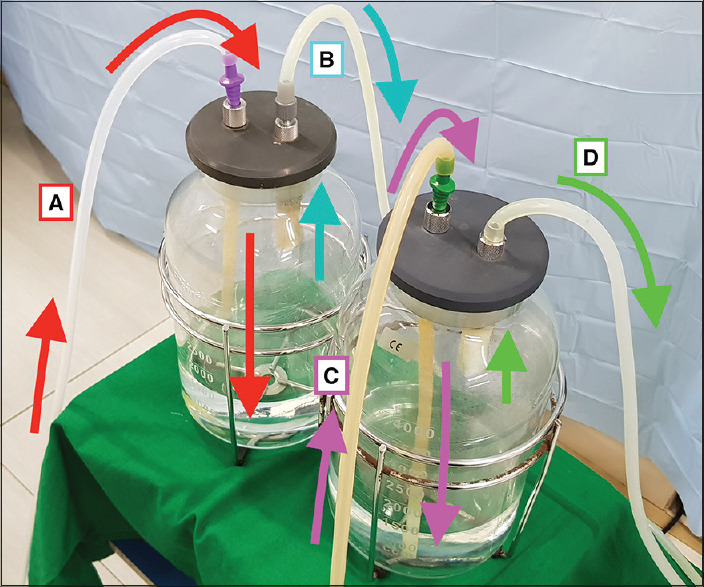
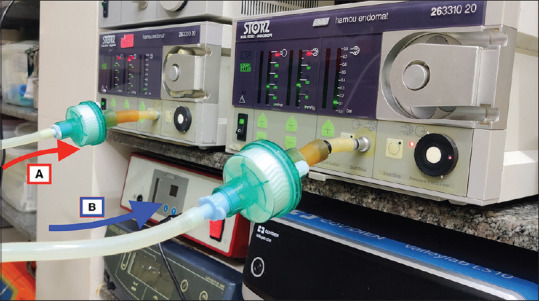
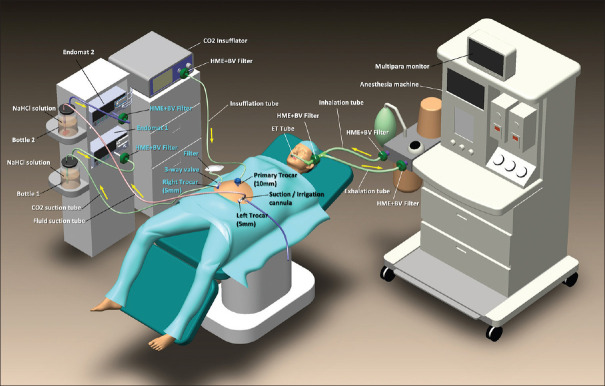
Materials and methods: Use of double closed circuit laparoscopic suction evacuation and filtration systems with closed circuit anaesthesia with specialized Heat and Moisture Exchangers (HME) bacterial & viral (BV) filters to make laparoscopic surgery safe.
Results: 57.14% of the patients were 41 years or more. 47.6% presented either with menorrhagia, irregular vaginal bleeding or post-menopausal vaginal bleeding and 26.19 % patients were keen to conceive. In 50% patients, surgery was done in 60 minutes or less. Post-operatively, none of the patients had any complications and all were followed up for 14 days for COVID-19 infection. No staff, doctors or anaesthetist were detected COVID-19 positive during the follow up period. The limitation of the study was, that it was an observational study done in COVID-19 negative patients only.
Conclusions: Safety at laparoscopy can be maintained when it is performed by an experienced surgeon who has full knowledge of safe laparoscopic techniques and performs it in the shortest time possible and with all due precautions.
Keywords: COVID-19; Laparoscopy; Minimally invasive surgery; SARS-CoV-2; Viral diffusion.
Copyright: © 2020 Journal of Human Reproductive Sciences.
Conflict of interest statement
There are no conflicts of interest.
Figures


Similar articles
-
Laparoscopic Gastrointestinal Surgery During COVID-19 Pandemic: Single-Center Experience.J Laparoendosc Adv Surg Tech A. 2021 Apr;31(4):455-457. doi: 10.1089/lap.2020.0481. Epub 2020 Aug 24. J Laparoendosc Adv Surg Tech A. 2021. PMID: 32915094
-
SARS-CoV-2 Prevalence in Laparoscopic Surgery Filters. Analysis in Patients with Negative Oropharyngeal RT-qPCR in a Pandemic Context: A Cross-Sectional Study.J Pers Med. 2021 Oct 20;11(11):1052. doi: 10.3390/jpm11111052. J Pers Med. 2021. PMID: 34834404 Free PMC article.
-
Emergency Abdominal Laparoscopic Surgery During the Coronavirus Disease 2019 Pandemic: Experience in a Private Center in Peru.J Laparoendosc Adv Surg Tech A. 2021 Mar;31(3):261-265. doi: 10.1089/lap.2020.0917. Epub 2020 Dec 14. J Laparoendosc Adv Surg Tech A. 2021. PMID: 33325786
-
Adaptations and Safety Modifications to Perform Safe Minimal Access Surgery (Minimally Invasive Surgery: Laparoscopy and Robotic) during the COVID-19 Pandemic.Surg Innov. 2021 Feb;28(1):123-133. doi: 10.1177/1553350620964323. Epub 2020 Oct 7. Surg Innov. 2021. PMID: 33026956 Free PMC article. Review.
-
Adaptations and Safety Modifications to Perform Safe Minimal Access Surgery (MIS: Laparoscopy and Robotic) During the COVID-19 Pandemic: Practice Modifications Expert Panel Consensus Guidelines from Academia of Minimal Access Surgical Oncology (AMASO).Indian J Surg Oncol. 2021 Apr;12(Suppl 1):210-220. doi: 10.1007/s13193-020-01254-9. Epub 2020 Nov 18. Indian J Surg Oncol. 2021. PMID: 33223748 Free PMC article. Review.
Cited by
-
The Impact of COVID-19 on Surgical Training: the Past, the Present and the Future.Indian J Surg. 2022 Apr;84(Suppl 1):131-138. doi: 10.1007/s12262-021-02964-2. Epub 2021 Jun 12. Indian J Surg. 2022. PMID: 34149230 Free PMC article.
-
Gynaecological Laparoscopic Surgeries in the Omicron Era: Improvising the Management Skills After Lessons Learnt From the Delta Wave.Cureus. 2022 Oct 4;14(10):e29904. doi: 10.7759/cureus.29904. eCollection 2022 Oct. Cureus. 2022. PMID: 36348863 Free PMC article.
References
-
- Cho K, Hogan C, Lee M, Biswas P, Landman J, Champault G, et al. Cells are present in the smoke created during laparoscopic surgery. Br J Surg. 1997;84:993–5. doi: 10.1002/bjs.1800840724. - PubMed
-
- Knolmayer TJ, Asbun HJ, Shibata G, Bowyer MW. An experimental model of cellular aerosolization during laparoscopic surgery. Surg Laparosc Endosc. 1977;7:399–402. - PubMed
-
- Ikramuddin S, Lucus J, Ellison EC, Schirmer WJ, Melvin WS. Detection of aerosolized cells during carbon dioxide laparoscopy. J Gastrointest Surg. 1998;2:580–3. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous