

Laparoscopic Bilateral Adrenalectomy in a Young Female Patient with Recurrent Cushing's Disease
- PMID: 33628530
- PMCID: PMC7895553
- DOI: 10.1155/2021/6632436
Laparoscopic Bilateral Adrenalectomy in a Young Female Patient with Recurrent Cushing's Disease
Abstract
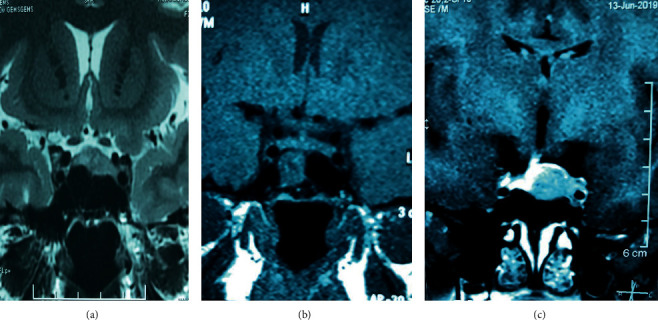
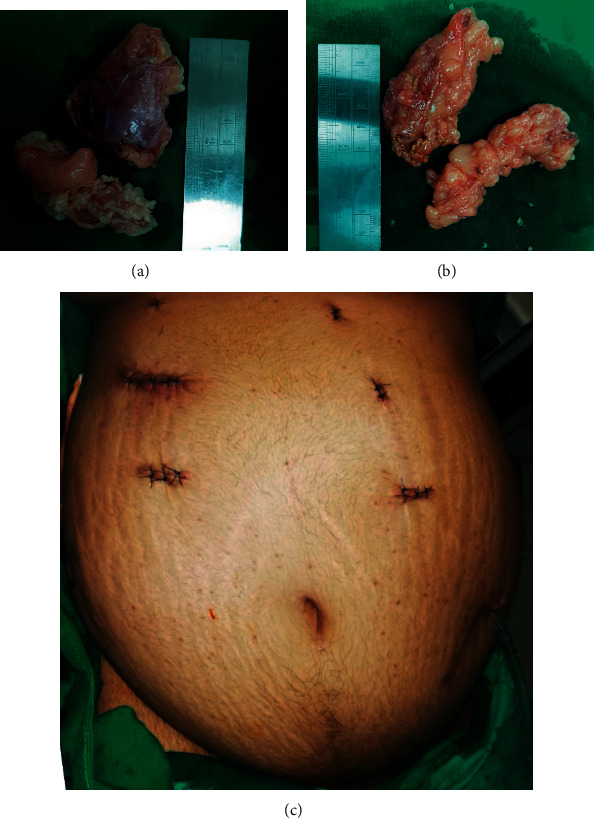
Introduction: Synchronous bilateral adrenalectomy is undertaken less often due to numerous perioperative challenges and rare circumstances of patients needing this procedure. Bilateral adrenalectomy is an important second-line option for patients with persistent or recurrent hypercortisolism following transsphenoidal surgery for Cushing's disease. Here, we present a challenging case of synchronous laparoscopic bilateral adrenalectomy for a young female patient with recurrent Cushing's disease and fertility wishes. Case Presentation. A 21-year-old recently married patient who was diagnosed with Cushing's disease with a pituitary microadenoma had undergone two attempts of transsphenoidal excision of the pituitary tumour. Follow-up evaluation showed an unresectable residual tumour with invasion of the intracavernous part of the left internal carotid artery. As the patient had the hypothalamic-pituitary-ovarian axis intact with strong fertility wishes, she was offered bilateral adrenalectomy instead of radiotherapy. She was prepared for the surgery with close perioperative support from the endocrinology and anaesthesia teams. Intravenous hydrocortisone infusion was started at the induction of anaesthesia. Transperitoneal approach was used with the patient positioned in left and right lateral positions for right and left glands, respectively. A meticulous surgical technique was used for the identification of adrenal veins to clip them before division followed by handling of the glands. The patient had minimal haemodynamic disturbances during surgery. Intraoperative blood loss was less than 100 ml, and operative time was 220 minutes. She had a gradual recovery following postoperative respiratory distress due to basal atelectasis and consolidation. Cortisol levels were less than 20 nmol/L postoperatively, suggesting successful surgical intervention. Two months after surgery, she continued on maintenance therapy of oral hydrocortisone and fludrocortisone and was encouraged to go ahead with pregnancy.
Conclusion: Although bilateral adrenalectomy is considered a high-risk procedure, these risks can be mitigated and performed safely while maintaining close multidisciplinary perioperative support.
Copyright © 2021 W. G. P. Kanchana et al.
Conflict of interest statement
All authors declare no conflicts of interest regarding the publication of the case report.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
