

High Prevalence of Multidrug-Resistant Clostridioides difficile Following Extensive Use of Antimicrobials in Hospitalized Patients in Kenya
- PMID: 33628744
- PMCID: PMC7897694
- DOI: 10.3389/fcimb.2020.604986
High Prevalence of Multidrug-Resistant Clostridioides difficile Following Extensive Use of Antimicrobials in Hospitalized Patients in Kenya
Abstract
Introduction: Clostridioides difficile is a neglected pathogen in many African countries as it is generally not regarded as one of the major contributors toward the diarrheal disease burden in the continent. However, several studies have suggested that C. difficile infection (CDI) may be underreported in many African settings. The aim of this study was to determine the prevalence of CDI in hospitalized patients, evaluate antimicrobial exposure, and detect toxin and antimicrobial resistance profiles of the isolated C. difficile strains.
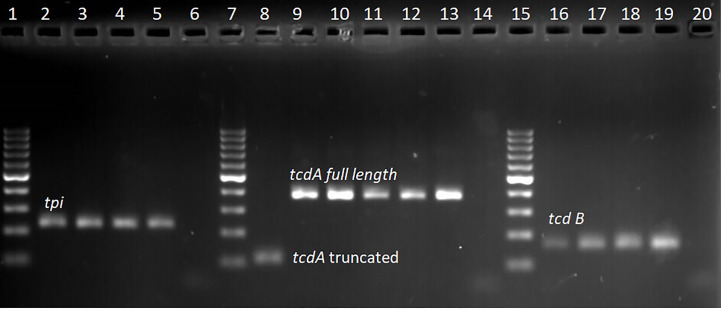
Methods: In this cross-sectional study, 333 hospitalized patients with hospital-onset diarrhoea were selected. The stool samples were collected and cultured on cycloserine-cefoxitin egg yolk agar (CCEY). Isolates were presumptively identified by phenotypic characteristics and Gram stain and confirmed by singleplex real-time PCR (qPCR) assays detecting the species-specific tpi gene, toxin A (tcdA) gene, toxin B (tcdB) gene, and the binary toxin (cdtA/cdtB) genes. Confirmed C. difficile isolates were tested against a panel of eight antimicrobials (vancomycin, metronidazole, rifampicin, ciprofloxacin, tetracycline, clindamycin, erythromycin, and ceftriaxone) using E-test strips.
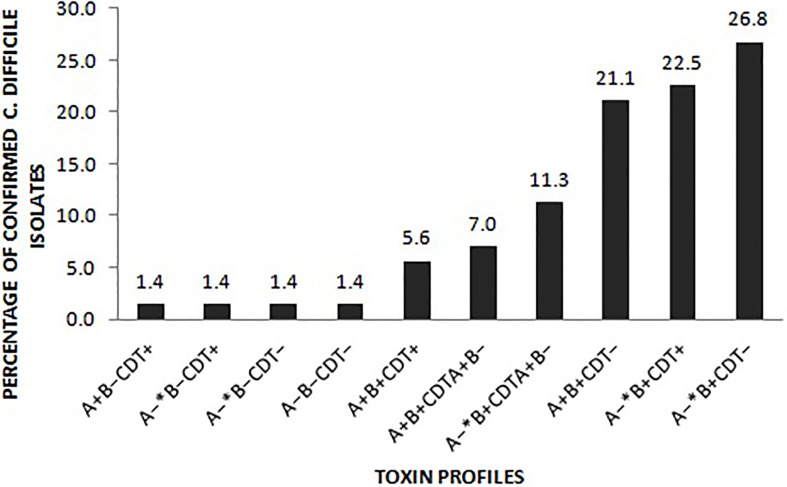
Results: C. difficile was detected in 57 (25%) of diarrheal patients over the age of two, 56 (98.2%) of whom received antimicrobials before the diarrheal episode. Amongst the 71 confirmed isolates, 69 (97.1%) harbored at least one toxin gene. More than half of the toxigenic isolates harbored a truncated tcdA gene. All isolates were sensitive to vancomycin, while three isolates (2.1%) were resistant to metronidazole (MIC >32 mg/L). High levels of resistance were observed to rifampicin (65/71, 91.5%), erythromycin (63/71, 88.7%), ciprofloxacin (59/71, 83.1%), clindamycin (57/71, 80.3%), and ceftriaxone (36/71, 50.7.8%). Among the resistant isolates, 61 (85.9%) were multidrug-resistant.
Conclusion: Multidrug-resistant C. difficile strains were a significant cause of healthcare facility-onset C. difficile infections in patients with prior antimicrobial exposure in this Kenyan hospital.
Keywords: Africa; Clostridioides difficile; antimicrobial use; multidrug resistance; toxin types.
Copyright © 2021 Mutai, Mureithi, Anzala, Revathi, Kullin, Burugu, Kyany’a, Odoyo, Otieno and Musila.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Clinical characteristics of community-onset Clostridioides difficile infections at a tertiary hospital in mainland China: A fourteen-year (2010-2023) retrospective study.Int J Med Microbiol. 2024 Sep;316:151631. doi: 10.1016/j.ijmm.2024.151631. Epub 2024 Jul 14. Int J Med Microbiol. 2024. PMID: 39024723
-
Study of the frequency of Clostridium difficile tcdA, tcdB, cdtA and cdtB genes in feces of Calves in south west of Iran.Ann Clin Microbiol Antimicrob. 2014 Jun 5;13:21. doi: 10.1186/1476-0711-13-21. Ann Clin Microbiol Antimicrob. 2014. PMID: 24903619 Free PMC article.
-
Frequency of toxin genes and antibiotic resistance pattern of Clostridioides difficile isolates in diarrheal samples among hospitalized patients in Hamadan, Iran.Gastroenterol Hepatol Bed Bench. 2021 Spring;14(2):165-173. Gastroenterol Hepatol Bed Bench. 2021. PMID: 33968344 Free PMC article.
-
Antimicrobial resistance in Clostridioides (Clostridium) difficile derived from humans: a systematic review and meta-analysis.Antimicrob Resist Infect Control. 2020 Sep 25;9(1):158. doi: 10.1186/s13756-020-00815-5. Antimicrob Resist Infect Control. 2020. PMID: 32977835 Free PMC article.
-
Prevalence and antimicrobial resistance pattern of Clostridium difficile among hospitalized diarrheal patients: A systematic review and meta-analysis.PLoS One. 2022 Jan 13;17(1):e0262597. doi: 10.1371/journal.pone.0262597. eCollection 2022. PLoS One. 2022. PMID: 35025959 Free PMC article.
Cited by
-
Antibiotic Resistance Profile of RT 027/176 Versus Other Clostridioides difficile Isolates in Silesia, Southern Poland.Pathogens. 2022 Aug 22;11(8):949. doi: 10.3390/pathogens11080949. Pathogens. 2022. PMID: 36015069 Free PMC article.
-
Characterization of Food Chain Clostridioides difficile Isolates in Terms of Ribotype and Antimicrobial Resistance.Microorganisms. 2023 May 16;11(5):1296. doi: 10.3390/microorganisms11051296. Microorganisms. 2023. PMID: 37317270 Free PMC article.
-
Probiotic use reduces the incidence of antibiotic-associated diarrhea among adult patients: a meta-analysis.Prz Gastroenterol. 2025;20(1):5-16. doi: 10.5114/pg.2025.148486. Epub 2025 Mar 16. Prz Gastroenterol. 2025. PMID: 40191517 Free PMC article. Review.
-
Global antibiotic use during the COVID-19 pandemic: analysis of pharmaceutical sales data from 71 countries, 2020-2022.EClinicalMedicine. 2023 Mar;57:101848. doi: 10.1016/j.eclinm.2023.101848. Epub 2023 Feb 6. EClinicalMedicine. 2023. PMID: 36776504 Free PMC article.
-
Vitamin D3 and carbamazepine protect against Clostridioides difficile infection in mice by restoring macrophage lysosome acidification.Autophagy. 2022 Sep;18(9):2050-2067. doi: 10.1080/15548627.2021.2016004. Epub 2022 Jan 6. Autophagy. 2022. PMID: 34989311 Free PMC article.
References
-
- Al-Barrak A., Embil J., Dyck B., Olekson K., Nicoll D., Alfa M., et al. (1999). An Outbreak of Toxin A Negative, Toxin B Positive Clostridium Difficile-Associated Diarrhea in a Canadian Tertiary-Care Hospital. Canada Commun. Dis. Rep. 25 (7), 65–69. - PubMed
-
- Beadsworth M. B. J., Keeley A. J., Roberts P., Farragher B., Watson A., Beeching N. J. (2014). Clostridium Difficile Toxin in Adult Inpatients in an Urban Hospital in Malawi: Associations with HIV Status, CD4 Count and Diarrhoea. Int. J. Trop. Med. 9 (1), 7–9. 10.4314/mmj.v28i2.8 - DOI
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
Miscellaneous