

Prognostic factors of resectable perihilar cholangiocarcinoma: a systematic review and meta-analysis of high-quality studies
- PMID: 33629062
- PMCID: PMC7882763
- DOI: 10.1177/2631774521993065
Prognostic factors of resectable perihilar cholangiocarcinoma: a systematic review and meta-analysis of high-quality studies
Abstract
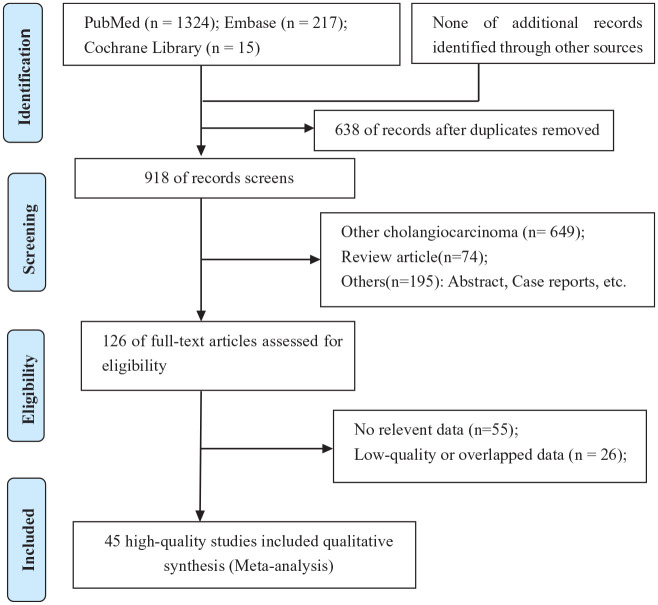
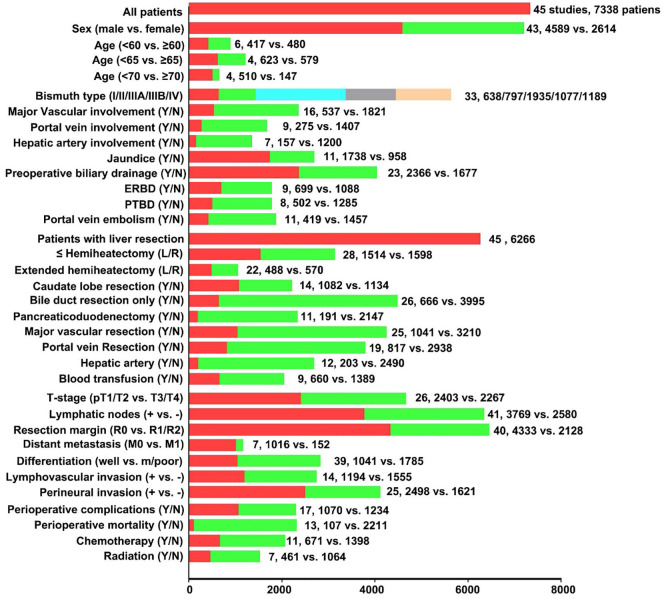
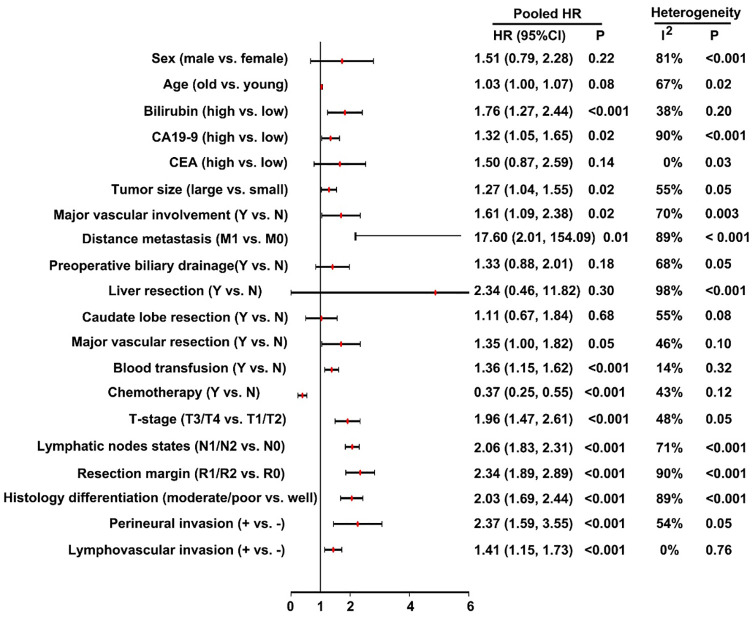
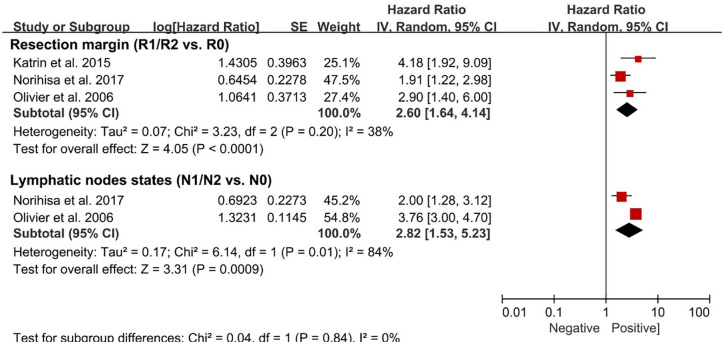
Data on prognostic factors associated with outcome following resection of perihilar cholangiocarcinoma vary. We sought to define and characterize current available evidence on prognostic factors associated with perihilar cholangiocarcinoma after resection. The PubMed, Embase, and Cochrane library were systematically searched for relevant studies published before December 2019. Prognostic factors were identified from multivariate regression analyses in studies. Only high-quality studies were included (Newcastle-Ottawa Scale > 6 stars). A total of 45 studies involving 7338 patients were analyzed. The meta-analysis demonstrated that serum bilirubin levels (hazard ratio: 1.76, 95% confidence interval: 1.27-2.44), serum CA19-9 levels (hazard ratio: 1.32, 95% confidence interval: 1.05-1.65), tumor size (hazard ratio: 1.27, 95% confidence interval: 1.04-1.55), major vascular involvement (hazard ratio: 1.61, 95% confidence interval: 1.09-2.38), distance metastasis (hazard ratio: 17.60, 95% confidence interval: 2.01-154.09), perioperative blood transfusion (hazard ratio: 1.36, 95% confidence interval: 1.15-1.62), T-stage (hazard ratio: 1.96, 95% confidence interval: 1.47-2.61), lymph node metastasis (hazard ratio: 2.06, 1.83-2.31), resection margin status (hazard ratio: 2.34, 95% confidence interval: 1.89-2.89), not-well histology differentiation (hazard ratio: 2.03, 95% confidence interval: 1.69-2.44), perineural invasion (hazard ratio: 2.37, 95% confidence interval: 1.59-3.55), and lymphovascular invasion (hazard ratio: 1.41, 95% confidence interval: 1.15-1.73) were prognostic factors for poorer overall survival. Adjuvant chemotherapy (hazard ratio: 0.37, 95% confidence interval: 0.25-0.55) had a positive effect on prolonged overall survival. In addition, positive resection margin status (hazard ratio: 1.96, 95% confidence interval: 1.47-2.61) and lymph node metastasis (hazard ratio: 2.06, 95% confidence interval: 1.83-2.31) were associated with poorer disease-free survival. The prognostic factors identified in the present meta-analysis can be used to characterize patients in clinical practice and enrich prognostic tools, which could be included in future trial designs and generate hypotheses to be tested in future research to promote personalized treatment.
Keywords: disease-free survival; overall survival; perihilar cholangiocarcinoma; prognostic factors; resection.
© The Author(s) 2021.
Conflict of interest statement
Conflict of interest statement: The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures
References
LinkOut - more resources
Full Text Sources
Other Literature Sources
