

Key Principles of Clinical Validation, Device Approval, and Insurance Coverage Decisions of Artificial Intelligence
- PMID: 33629545
- PMCID: PMC7909857
- DOI: 10.3348/kjr.2021.0048
Key Principles of Clinical Validation, Device Approval, and Insurance Coverage Decisions of Artificial Intelligence
Abstract
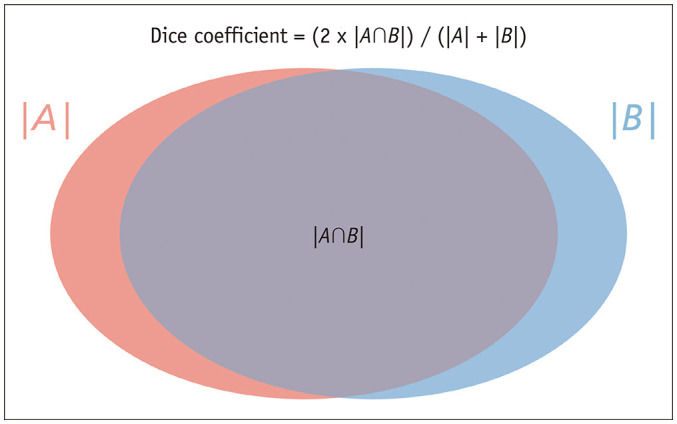
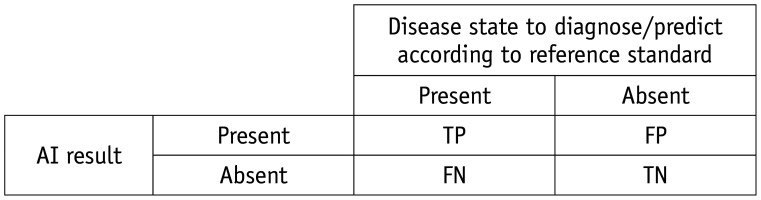
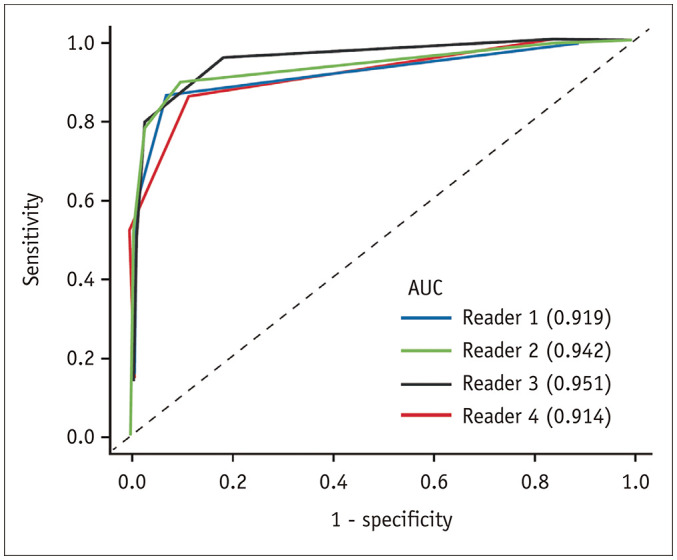
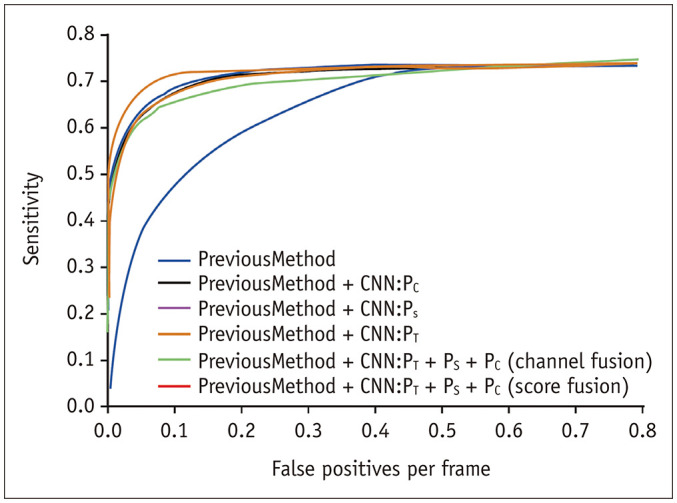
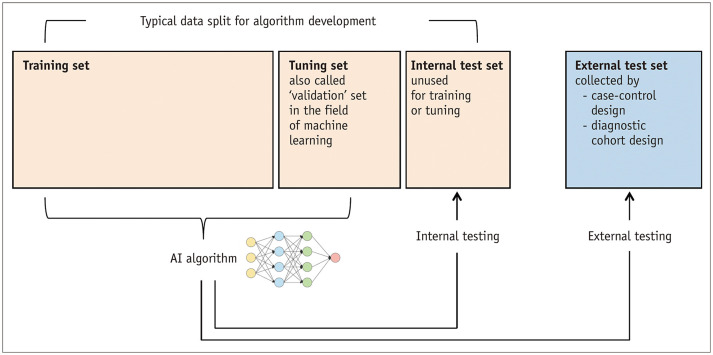
Artificial intelligence (AI) will likely affect various fields of medicine. This article aims to explain the fundamental principles of clinical validation, device approval, and insurance coverage decisions of AI algorithms for medical diagnosis and prediction. Discrimination accuracy of AI algorithms is often evaluated with the Dice similarity coefficient, sensitivity, specificity, and traditional or free-response receiver operating characteristic curves. Calibration accuracy should also be assessed, especially for algorithms that provide probabilities to users. As current AI algorithms have limited generalizability to real-world practice, clinical validation of AI should put it to proper external testing and assisting roles. External testing could adopt diagnostic case-control or diagnostic cohort designs. A diagnostic case-control study evaluates the technical validity/accuracy of AI while the latter tests the clinical validity/accuracy of AI in samples representing target patients in real-world clinical scenarios. Ultimate clinical validation of AI requires evaluations of its impact on patient outcomes, referred to as clinical utility, and for which randomized clinical trials are ideal. Device approval of AI is typically granted with proof of technical validity/accuracy and thus does not intend to directly indicate if AI is beneficial for patient care or if it improves patient outcomes. Neither can it categorically address the issue of limited generalizability of AI. After achieving device approval, it is up to medical professionals to determine if the approved AI algorithms are beneficial for real-world patient care. Insurance coverage decisions generally require a demonstration of clinical utility that the use of AI has improved patient outcomes.
Keywords: Artificial intelligence; Device approval; Insurance coverage; Software validation.
Copyright © 2021 The Korean Society of Radiology.
Conflict of interest statement
The authors have no potential conflicts of interest to disclose.
Figures
Similar articles
-
Survey on Value Elements Provided by Artificial Intelligence and Their Eligibility for Insurance Coverage With an Emphasis on Patient-Centered Outcomes.Korean J Radiol. 2024 May;25(5):414-425. doi: 10.3348/kjr.2023.1281. Epub 2024 Mar 20. Korean J Radiol. 2024. PMID: 38627874 Free PMC article.
-
The development an artificial intelligence algorithm for early sepsis diagnosis in the intensive care unit.Int J Med Inform. 2020 Sep;141:104176. doi: 10.1016/j.ijmedinf.2020.104176. Epub 2020 May 21. Int J Med Inform. 2020. PMID: 32485555
-
What Are the Applications and Limitations of Artificial Intelligence for Fracture Detection and Classification in Orthopaedic Trauma Imaging? A Systematic Review.Clin Orthop Relat Res. 2019 Nov;477(11):2482-2491. doi: 10.1097/CORR.0000000000000848. Clin Orthop Relat Res. 2019. PMID: 31283727 Free PMC article.
-
Design Characteristics of Studies Reporting the Performance of Artificial Intelligence Algorithms for Diagnostic Analysis of Medical Images: Results from Recently Published Papers.Korean J Radiol. 2019 Mar;20(3):405-410. doi: 10.3348/kjr.2019.0025. Korean J Radiol. 2019. PMID: 30799571 Free PMC article.
-
An Innovative Artificial Intelligence-Based App for the Diagnosis of Gestational Diabetes Mellitus (GDM-AI): Development Study.J Med Internet Res. 2020 Sep 15;22(9):e21573. doi: 10.2196/21573. J Med Internet Res. 2020. PMID: 32930674 Free PMC article.
Cited by
-
Ethical Considerations in the Use of Artificial Intelligence and Machine Learning in Health Care: A Comprehensive Review.Cureus. 2024 Jun 15;16(6):e62443. doi: 10.7759/cureus.62443. eCollection 2024 Jun. Cureus. 2024. PMID: 39011215 Free PMC article. Review.
-
The risks of artificial intelligence: A narrative review and ethical reflection from an Oral Medicine group.Oral Dis. 2025 Feb;31(2):348-353. doi: 10.1111/odi.15100. Epub 2024 Aug 23. Oral Dis. 2025. PMID: 39176474 Free PMC article. Review.
-
[Applications of Artificial Intelligence in Mammography from a Development and Validation Perspective].Taehan Yongsang Uihakhoe Chi. 2021 Jan;82(1):12-28. doi: 10.3348/jksr.2020.0205. Epub 2021 Jan 31. Taehan Yongsang Uihakhoe Chi. 2021. PMID: 36237466 Free PMC article. Review. Korean.
-
Artificial intelligence in atrial fibrillation: emerging applications, research directions and ethical considerations.Front Cardiovasc Med. 2025 Jun 24;12:1596574. doi: 10.3389/fcvm.2025.1596574. eCollection 2025. Front Cardiovasc Med. 2025. PMID: 40630898 Free PMC article. Review.
-
Looking Ahead to 2022 for the Korean Journal of Radiology.Korean J Radiol. 2022 Jan;23(1):6-9. doi: 10.3348/kjr.2021.0844. Korean J Radiol. 2022. PMID: 34983089 Free PMC article. No abstract available.
References
-
- Topol EJ. High-performance medicine: the convergence of human and artificial intelligence. Nat Med. 2019;25:44–56. - PubMed
-
- Park SH, Lim TH. Artificial intelligence: guide for healthcare personnel. Seoul: Koonja; 2020.
-
- Choi JS, Han BK, Ko ES, Bae JM, Ko EY, Song SH, et al. Effect of a deep learning framework-based computer-aided diagnosis system on the diagnostic performance of radiologists in differentiating between malignant and benign masses on breast ultrasonography. Korean J Radiol. 2019;20:749–758. - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
