

Assessment of Clinical Benefit of Integrative Genomic Profiling in Advanced Solid Tumors
- PMID: 33630025
- PMCID: PMC7907987
- DOI: 10.1001/jamaoncol.2020.7987
Assessment of Clinical Benefit of Integrative Genomic Profiling in Advanced Solid Tumors
Abstract
Importance: Use of next-generation sequencing (NGS) to identify clinically actionable genomic targets has been incorporated into routine clinical practice in the management of advanced solid tumors; however, the clinical utility of this testing remains uncertain.
Objective: To determine which patients derived the greatest degree of clinical benefit from NGS profiling.
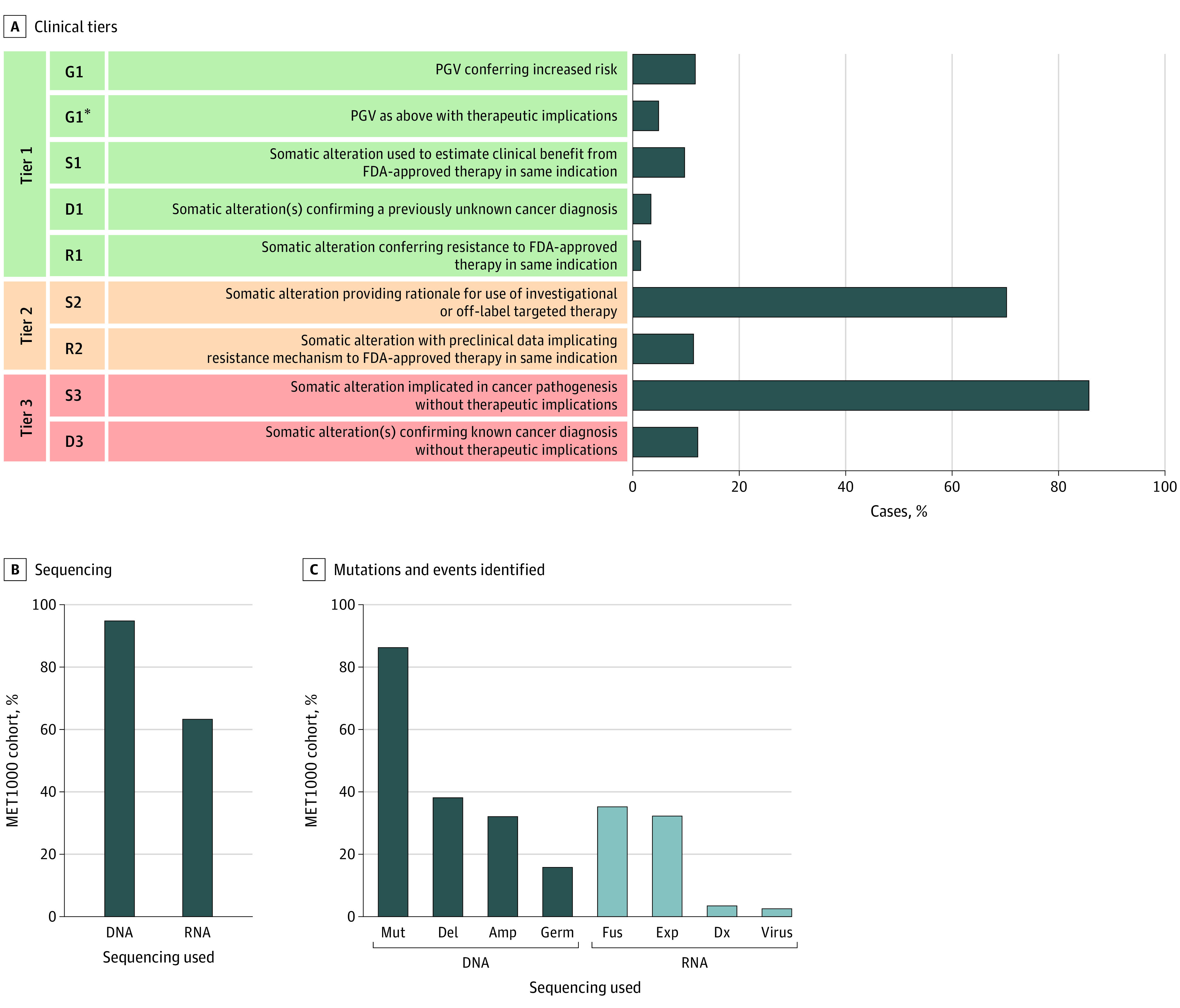
Design, setting, and participants: Patients in this cohort study underwent fresh tumor biopsy and blood sample collection for genomic profiling of paired tumor and normal DNA (whole-exome or targeted-exome capture with analysis of 1700 genes) and tumor transcriptome (RNA) sequencing. Somatic and germline genomic alterations were annotated and classified according to degree of clinical actionability. Results were returned to treating oncologists. Data were collected from May 1, 2011, to February 28, 2018, and analyzed from May 1, 2011, to April 30, 2020.
Main outcomes and measures: Patients' subsequent therapy and treatment response were extracted from the medical record to determine clinical benefit rate from NGS-directed therapy at 6 months and exceptional responses lasting 12 months or longer.
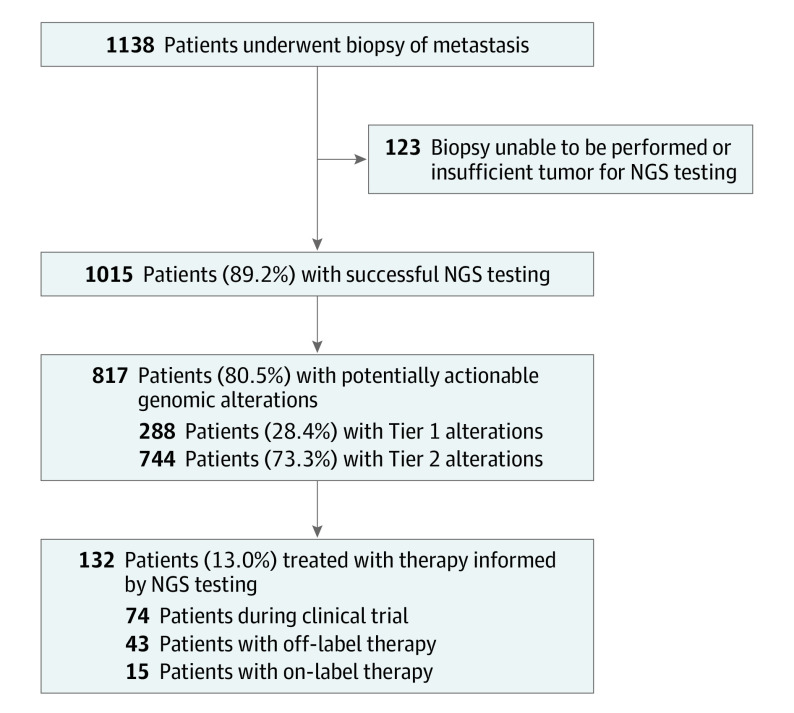
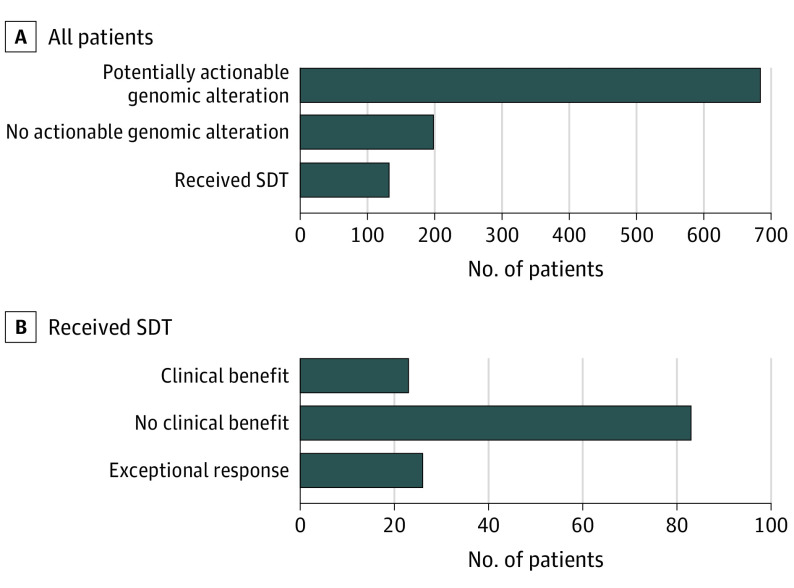
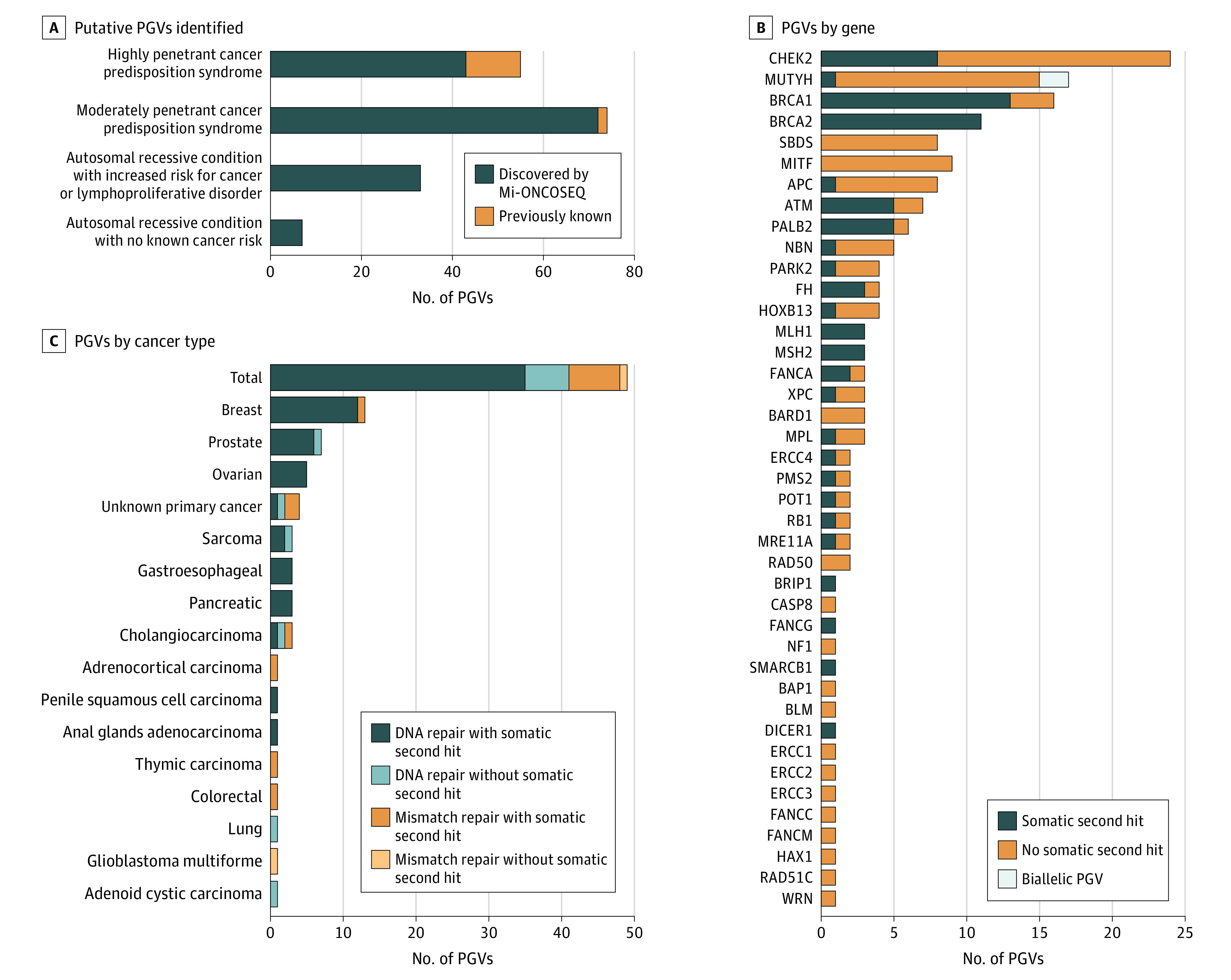
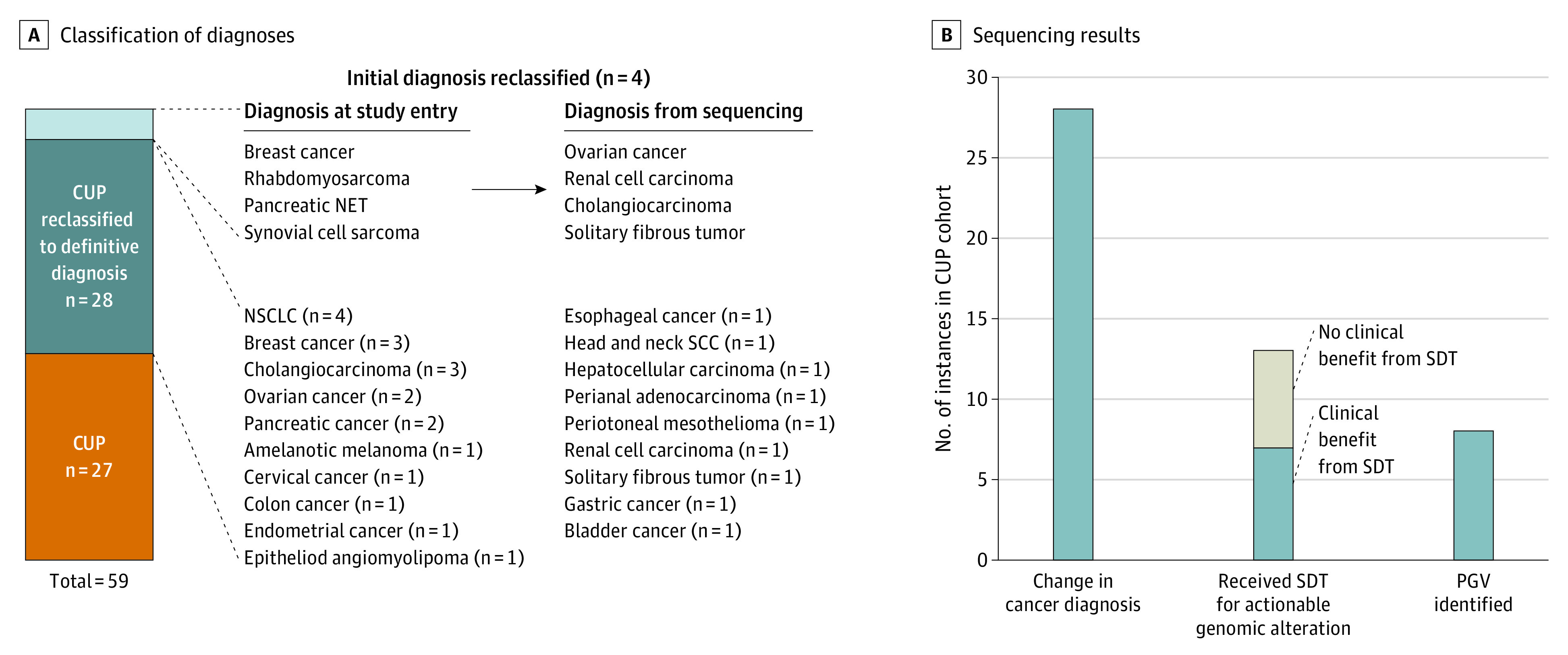
Results: During the study period, NGS was attempted on tumors from 1138 patients and was successful in 1015 (89.2%) (MET1000 cohort) (538 men [53.0%]; mean [SD] age, 57.7 [13.3] years). Potentially clinically actionable genomic alterations were discovered in 817 patients (80.5%). Of these, 132 patients (16.2%) received sequencing-directed therapy, and 49 had clinical benefit (37.1%). Exceptional responses were observed in 26 patients (19.7% of treated patients). Pathogenic germline variants (PGVs) were identified in 160 patients (15.8% of cohort), including 49 PGVs (4.8% of cohort) with therapeutic relevance. For 55 patients with carcinoma of unknown primary origin, NGS identified the primary site in 28 (50.9%), and sequencing-directed therapy in 13 patients resulted in clinical benefit in 7 instances (53.8%), including 5 exceptional responses.
Conclusions and relevance: The high rate of therapeutically relevant PGVs identified across diverse cancer types supports a recommendation for directed germline testing in all patients with advanced cancer. The high frequency of therapeutically relevant somatic and germline findings in patients with carcinoma of unknown primary origin and other rare cancers supports the use of comprehensive NGS profiling as a component of standard of care for these disease entities.
Conflict of interest statement
Figures
Comment in
-
Precision Medicine in Oncology-Toward the Integrated Targeting of Somatic and Germline Genomic Aberrations.JAMA Oncol. 2021 Apr 1;7(4):507-509. doi: 10.1001/jamaoncol.2020.7988. JAMA Oncol. 2021. PMID: 33630035 No abstract available.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
