

Sex Differences in Cognitive Decline Among US Adults
- PMID: 33630089
- PMCID: PMC7907956
- DOI: 10.1001/jamanetworkopen.2021.0169
Sex Differences in Cognitive Decline Among US Adults
Erratum in
-
Error in Methods.JAMA Netw Open. 2023 Mar 1;6(3):e234786. doi: 10.1001/jamanetworkopen.2023.4786. JAMA Netw Open. 2023. PMID: 36877526 Free PMC article. No abstract available.
Abstract
Importance: Sex differences in dementia risk are unclear, but some studies have found greater risk for women.
Objective: To determine associations between sex and cognitive decline in order to better understand sex differences in dementia risk.
Design, setting, and participants: This cohort study used pooled analysis of individual participant data from 5 cohort studies for years 1971 to 2017: Atherosclerosis Risk in Communities Study, Coronary Artery Risk Development in Young Adults Study, Cardiovascular Health Study, Framingham Offspring Study, and Northern Manhattan Study. Linear mixed-effects models were used to estimate changes in each continuous cognitive outcome over time by sex. Data analysis was completed from March 2019 to October 2020.
Exposure: Sex.
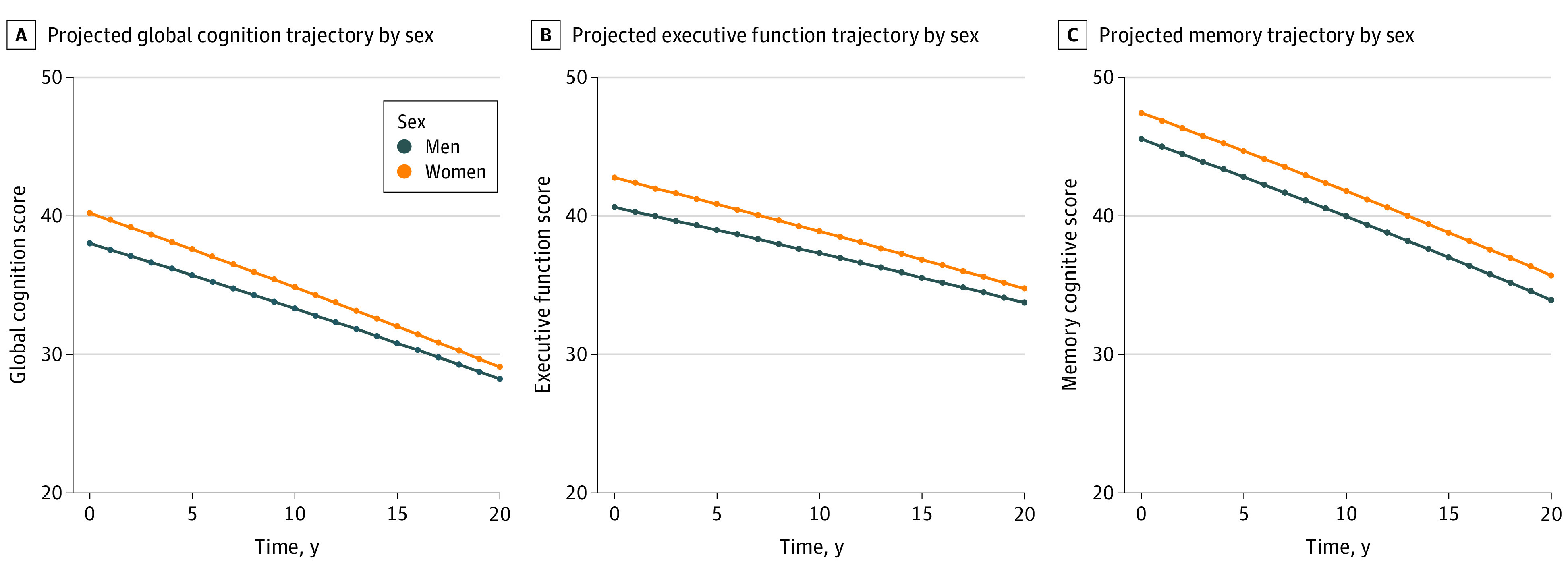
Main outcomes and measures: The primary outcome was change in global cognition. Secondary outcomes were change in memory and executive function. Outcomes were standardized as t scores (mean [SD], 50 [10]); a 1-point difference represents a 0.1-SD difference in cognition.
Results: Among 34 349 participants, 26 088 who self-reported Black or White race, were free of stroke and dementia, and had covariate data at or before the first cognitive assessment were included for analysis. Median (interquartile range) follow-up was 7.9 (5.3-20.5) years. There were 11 775 (44.7%) men (median [interquartile range] age, 58 [51-66] years at first cognitive assessment; 2229 [18.9%] Black) and 14 313 women (median [interquartile range] age, 58 [51-67] years at first cognitive assessment; 3636 [25.4%] Black). Women had significantly higher baseline performance than men in global cognition (2.20 points higher; 95% CI, 2.04 to 2.35 points; P < .001), executive function (2.13 points higher; 95% CI, 1.98 to 2.29 points; P < .001), and memory (1.89 points higher; 95% CI, 1.72 to 2.06 points; P < .001). Compared with men, women had significantly faster declines in global cognition (-0.07 points/y faster; 95% CI, -0.08 to -0.05 points/y; P < .001) and executive function (-0.06 points/y faster; 95% CI, -0.07 to -0.05 points/y; P < .001). Men and women had similar declines in memory (-0.004 points/y faster; 95% CI, -0.023 to 0.014; P = .61).
Conclusions and relevance: The results of this cohort study suggest that women may have greater cognitive reserve but faster cognitive decline than men, which could contribute to sex differences in late-life dementia.
Conflict of interest statement
Figures

References
-
- Alzheimer's Association . 2020 Alzheimer's Disease facts and figures. Alzheimers Dement. 2020;16(3):391-460. doi: 10.1002/alz.12068 - DOI
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
