

The cost-effectiveness of prostate cancer screening using the Stockholm3 test
- PMID: 33630863
- PMCID: PMC7906342
- DOI: 10.1371/journal.pone.0246674
The cost-effectiveness of prostate cancer screening using the Stockholm3 test
Abstract
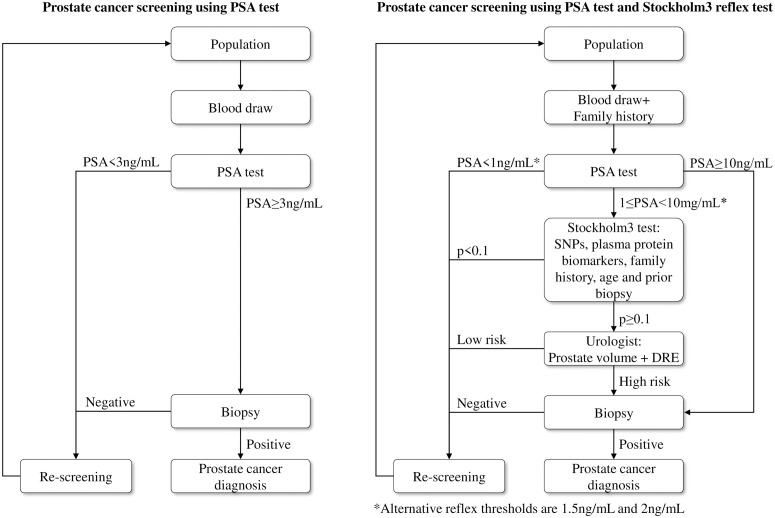
Objectives: The European Randomized Study of Screening for Prostate Cancer found that prostate-specific antigen (PSA) screening reduced prostate cancer mortality, however the costs and harms from screening may outweigh any mortality reduction. Compared with screening using the PSA test alone, using the Stockholm3 Model (S3M) as a reflex test for PSA ≥ 1 ng/mL has the same sensitivity for Gleason score ≥ 7 cancers while the relative positive fractions for Gleason score 6 cancers and no cancer were 0.83 and 0.56, respectively. The cost-effectiveness of the S3M test has not previously been assessed.
Methods: We undertook a cost-effectiveness analysis from a lifetime societal perspective. Using a microsimulation model, we simulated for: (i) no prostate cancer screening; (ii) screening using the PSA test; and (iii) screening using the S3M test as a reflex test for PSA values ≥ 1, 1.5 and 2 ng/mL. Screening strategies included quadrennial re-testing for ages 55-69 years performed by a general practitioner. Discounted costs, quality-adjusted life-years (QALYs) and incremental cost-effectiveness ratios (ICERs) were calculated.
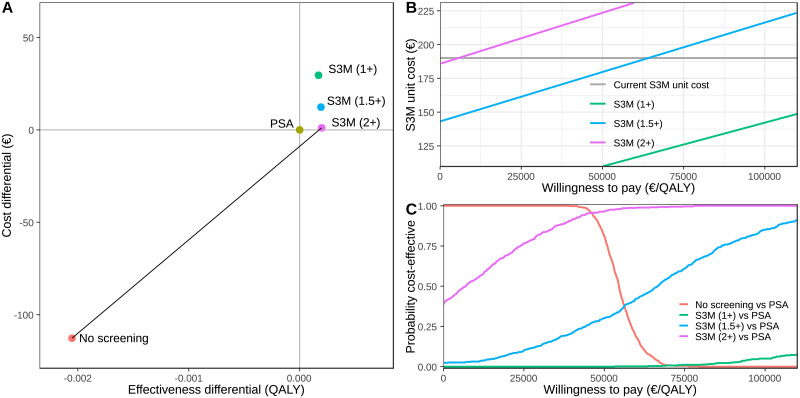
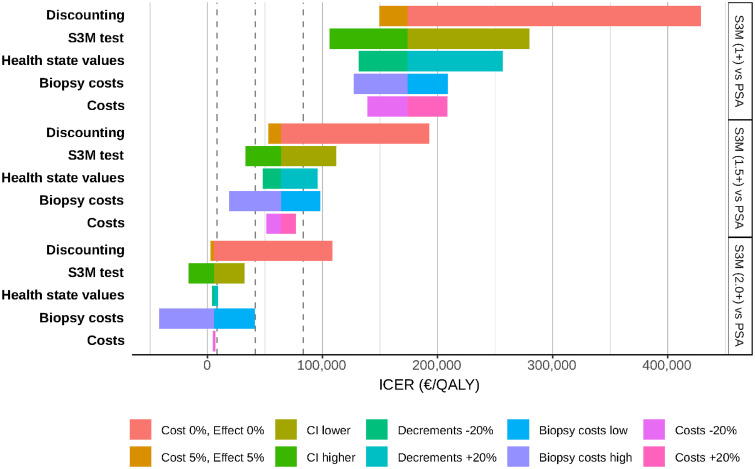
Results: Comparing S3M with a reflex threshold of 2 ng/mL with screening using the PSA test, S3M had increased effectiveness, reduced lifetime biopsies by 30%, and increased societal costs by 0.4%. Relative to the PSA test, the S3M reflex thresholds of 1, 1.5 and 2 ng/mL had ICERs of 170,000, 60,000 and 6,000 EUR/QALY, respectively. The S3M test was more cost-effective at higher biopsy costs.
Conclusions: Prostate cancer screening using the S3M test for men with an initial PSA ≥ 2.0 ng/mL was cost-effective compared with screening using the PSA test alone.
Conflict of interest statement
MC, TN and LE were investigators on the Stockholm3 trial. They and the other authors have no financial or any other conflicts of interest. Specifically, none of the authors are party to the intellectual property associated with the Stockholm3 test. Author AJ is a full time employee and shareholder of AstraZeneca. AstraZeneca provided support in the form of salary for author AJ, but did not have any additional role in the study design, data collection and analysis, decision to publish, or preparation of the manuscript. The competing interests declared do not alter our adherence to PLOS ONE policies on sharing data and materials.
Figures
Similar articles
-
Cost-Effectiveness of the Stockholm3 Test and Magnetic Resonance Imaging in Prostate Cancer Screening: A Microsimulation Study.Eur Urol. 2022 Jul;82(1):12-19. doi: 10.1016/j.eururo.2021.12.021. Epub 2022 Jan 31. Eur Urol. 2022. PMID: 35094896
-
The Stockholm-3 Model for Prostate Cancer Detection: Algorithm Update, Biomarker Contribution, and Reflex Test Potential.Eur Urol. 2018 Aug;74(2):204-210. doi: 10.1016/j.eururo.2017.12.028. Epub 2018 Jan 10. Eur Urol. 2018. PMID: 29331214
-
The Cost-Effectiveness of Prostate Cancer Detection with the Use of Prostate Health Index.Value Health. 2016 Mar-Apr;19(2):153-7. doi: 10.1016/j.jval.2015.12.002. Epub 2016 Jan 14. Value Health. 2016. PMID: 27021748
-
Prostate-Specific Antigen (PSA)-Based Population Screening for Prostate Cancer: An Economic Analysis.Ont Health Technol Assess Ser. 2015 May 1;15(11):1-37. eCollection 2015. Ont Health Technol Assess Ser. 2015. PMID: 26366237 Free PMC article. Review.
-
Assessment of prostate-specific antigen screening: an evidence-based report by the German Institute for Quality and Efficiency in Health Care.BJU Int. 2022 Mar;129(3):280-289. doi: 10.1111/bju.15444. Epub 2021 Jul 7. BJU Int. 2022. PMID: 33961337 Review.
Cited by
-
Economic evaluation of prostate cancer risk assessment methods: A cost-effectiveness analysis using population data.Cancer Med. 2023 Oct;12(19):20106-20118. doi: 10.1002/cam4.6587. Epub 2023 Sep 23. Cancer Med. 2023. PMID: 37740609 Free PMC article.
-
Systematic Review on the Cost Effectiveness of Prostate Cancer Screening in Europe.Eur Urol. 2024 Nov;86(5):400-408. doi: 10.1016/j.eururo.2024.04.036. Epub 2024 May 23. Eur Urol. 2024. PMID: 38789306 Free PMC article.
-
The Cost Effectiveness of Genomic Medicine in Cancer Control: A Systematic Literature Review.Appl Health Econ Health Policy. 2025 May;23(3):359-393. doi: 10.1007/s40258-025-00949-w. Epub 2025 Mar 29. Appl Health Econ Health Policy. 2025. PMID: 40172779 Free PMC article.
-
Design and Implementation of Taizhou Integrated Prostate Screening.Am J Mens Health. 2022 Nov-Dec;16(6):15579883221138192. doi: 10.1177/15579883221138192. Am J Mens Health. 2022. PMID: 36412060 Free PMC article.
-
Cost-Effectiveness Analysis of Stockholm 3 Testing Compared to PSA as the Primary Blood Test in the Prostate Cancer Diagnostic Pathway: A Decision Tree Approach.Appl Health Econ Health Policy. 2022 Nov;20(6):867-880. doi: 10.1007/s40258-022-00741-0. Epub 2022 Aug 8. Appl Health Econ Health Policy. 2022. PMID: 35934771 Free PMC article.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
