

Effects of therapeutic hypothermia on death among asphyxiated neonates with hypoxic-ischemic encephalopathy: A systematic review and meta-analysis of randomized control trials
- PMID: 33630892
- PMCID: PMC7906350
- DOI: 10.1371/journal.pone.0247229
Effects of therapeutic hypothermia on death among asphyxiated neonates with hypoxic-ischemic encephalopathy: A systematic review and meta-analysis of randomized control trials
Abstract
Background: Hypoxic perinatal brain injury is caused by lack of oxygen to baby's brain and can lead to death or permanent brain damage. However, the effectiveness of therapeutic hypothermia in birth asphyxiated infants with encephalopathy is uncertain. This systematic review and meta-analysis was aimed to estimate the pooled relative risk of mortality among birth asphyxiated neonates with hypoxic-ischemic encephalopathy in a global context.
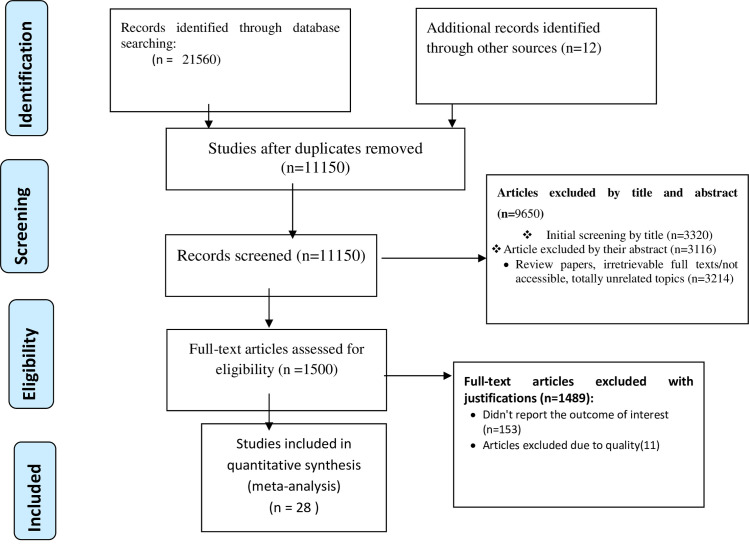
Methods: We used the Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) guidelines to search randomized control trials from electronic databases (PubMed, Cochrane library, Google Scholar, MEDLINE, Embase, Scopus, Web of Science, Cochrane Central Register of Controlled Trials (CENTRAL), and meta register of Current Controlled Trials (mCRT)). The authors extracted the author's name, year of publication, country, method of cooling, the severity of encephalopathy, the sample size in the hypothermic, and non-hypothermic groups, and the number of deaths in the intervention and control groups. A weighted inverse variance fixed-effects model was used to estimate the pooled relative risk of mortality. The subgroup analysis was done by economic classification of countries, methods of cooling, and cooling devices. Publication bias was assessed with a funnel plot and Eggers test. A sensitivity analysis was also done.
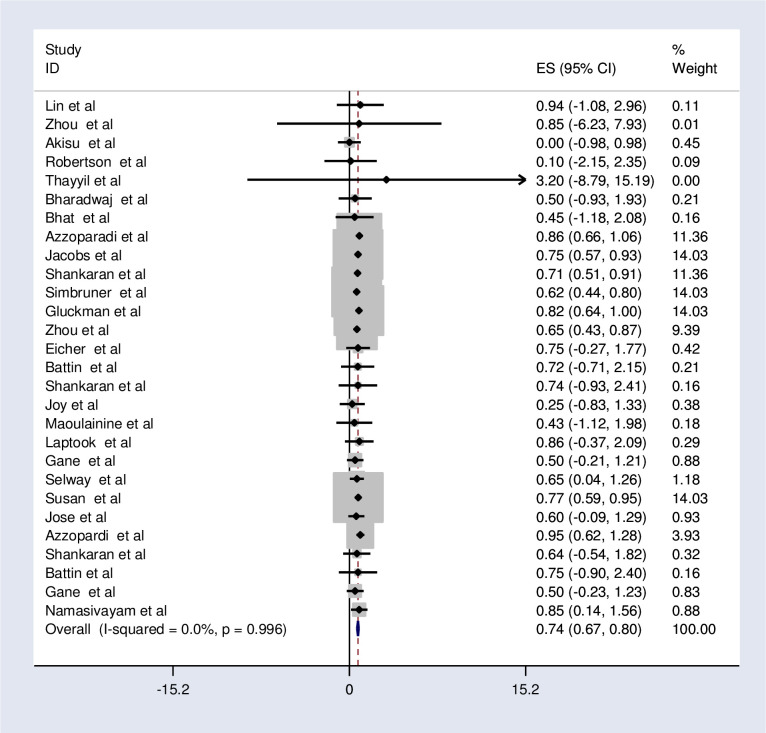
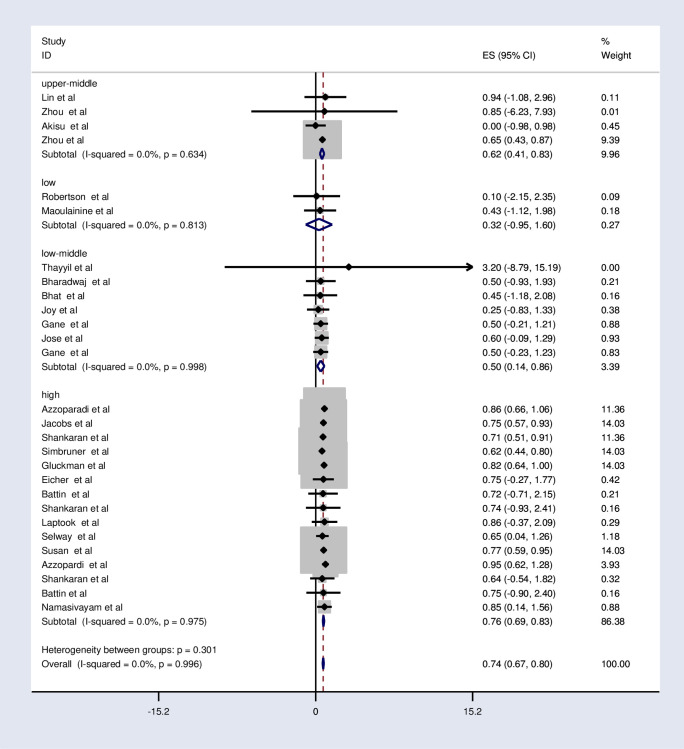
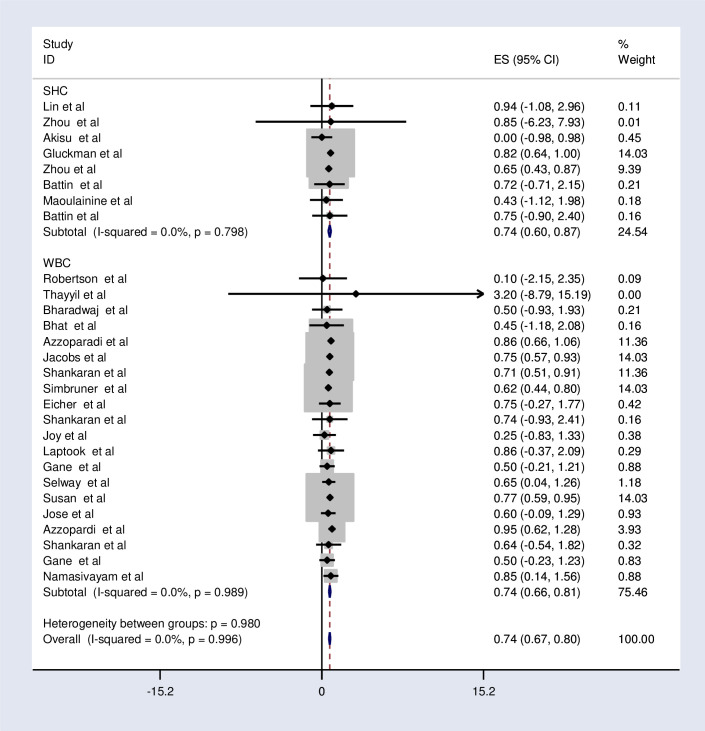
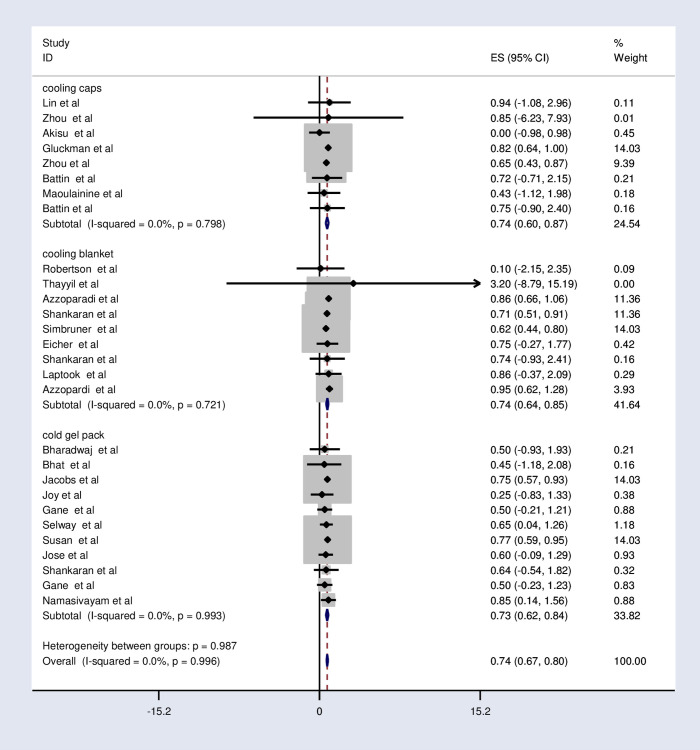
Results: A total of 28 randomized control trials with a total sample of 35, 92 (1832 hypothermic 1760 non-hypothermic) patients with hypoxic-ischemic encephalopathy were used for the analysis. The pooled relative risk of mortality after implementation of therapeutic hypothermia was found to be 0.74 (95%CI; 0.67, 0.80; I2 = 0.0%; p<0.996). The subgroup analysis revealed that the pooled relative risk of mortality in low, low middle, upper-middle and high income countries was 0.32 (95%CI; -0.95, 1.60; I2 = 0.0%; p<0.813), 0.5 (95%CI; 0.14, 0.86; I2 = 0.0%; p<0.998), 0.62 (95%CI; 0.41-0.83; I2 = 0.0%; p<0.634) and 0.76 (95%CI; 0.69-0.83; I2 = 0.0%; p<0.975) respectively. The relative risk of mortality was the same in selective head cooling and whole-body cooling method which was 0.74. Regarding the cooling device, the pooled relative risk of mortality is the same between the cooling cap and cooling blanket (0.74). However, it is slightly lower (0.73) in a cold gel pack.
Conclusions: Therapeutic hypothermia reduces the risk of death in neonates with moderate to severe hypoxic-ischemic encephalopathy. Both selective head cooling and whole-body cooling method are effective in reducing the mortality of infants with this condition. Moreover, low income countries benefit the most from the therapy. Therefore, health professionals should consider offering therapeutic hypothermia as part of routine clinical care to newborns with hypoxic-ischemic encephalopathy especially in low-income countries.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Prof.-Aggrey-Wasunna.pdf. Neonatal Therapeutic hypothermia. http://wwwkenyapaediatricorg/. 2018.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
