

Comparison of chest radiography and chest CT for evaluation of pediatric COVID-19 pneumonia: Does CT add diagnostic value?
- PMID: 33631061
- PMCID: PMC8014659
- DOI: 10.1002/ppul.25313
Comparison of chest radiography and chest CT for evaluation of pediatric COVID-19 pneumonia: Does CT add diagnostic value?
Abstract
Purpose: First, to investigate the added diagnostic value of chest computed tomography (CT) for evaluating COVID-19 in symptomatic children by comparing chest CT findings with chest radiographic findings, and second, to identify the imaging signs and patterns on CT associated with COVID-19 pneumonia in children.
Materials and methods: From March 2020 to December 2020, 56 consecutive children (33 males and 23 girls; mean age ± SD, 14.8 ± 5.0 years; range, 9 months-18 years) with mild to moderate symptom and laboratory confirmed COVID-19 (based on Centers for Disease Control criteria) underwent both chest radiography and chest CT on the same day within the first 2 days of initial presentation to the hospital. Two experienced radiologists independently evaluated chest radiographs and chest CT studies for thoracic abnormalities. The findings from chest radiography and chest CT were compared to evaluate the added diagnostic value of chest CT for affecting patient management. Interobserver agreement was measured with Cohen's κ statistics.
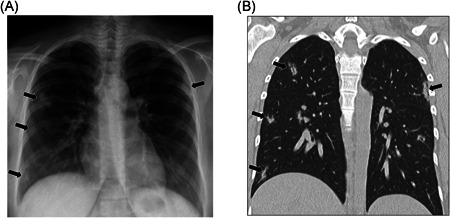
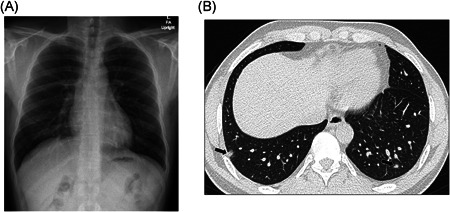
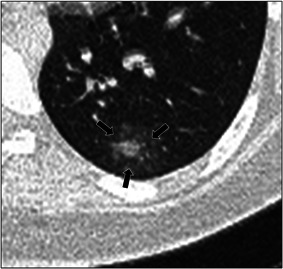
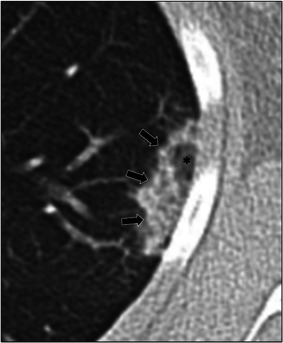
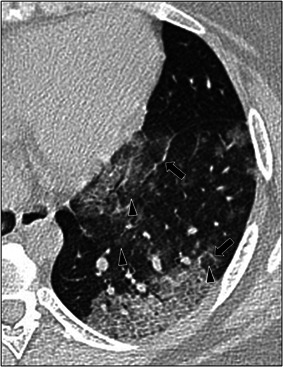
Results: Eleven (19.6%) of 56 patients had abnormal chest radiographic findings, including ground-glass opacity (GGO) in 5/11 (45.4%) and combined GGO and consolidation in 6/11 (54.5%). On chest CT, 26 (46.4%) of 56 patients had abnormal CT findings, including combined GGO and consolidation in 19/26 (73.1%), GGO in 6/26 (23.1%), and consolidation in 1/26 (3.8%). Chest CT detected all thoracic abnormalities seen on chest radiography in 11/26 (42.3%) cases. In 15/26 (57.7%), chest CT detected lung abnormalities that were not observed on chest radiography, which included GGO and consolidation in 9/15 (60%), GGO in 5/15 (33.3%), and consolidation in 1/15 (6.6%) cases. These additional CT findings did not affect patient management. In addition, chest CT detected radiological signs and patterns, including the halo sign, reversed halo sign, crazy paving pattern, and tree-in-bud pattern. There was almost perfect interobserver agreement between the two reviewers for detecting findings on both chest radiographs (κ, 0.89, p = .001) and chest CT (κ, 0.96, p = .001) studies.
Conclusion: Chest CT detected lung abnormalities, including GGO and/or consolidation, that were not observed on chest radiography in more than half of symptomatic pediatric patients with COVID-19 pneumonia. However, these additional CT findings did not affect patient management. Therefore, CT is not clinically indicated for the initial evaluation of mild to moderately symptomatic pediatric patients with COVID-19 pneumonia.
Keywords: COVID-19 pneumonia; children; computed tomography; pediatric patients; radiography.
© 2021 Wiley Periodicals LLC.
Figures

References
-
- Foust AM, Johnston PR, Kasznia‐Brown J, et al. Perceived impact of COVID‐19 on pediatric radiology departments around the world: WFPI COVID‐19 Task Force survey results from 6 continents [published online ahead of print September 17, 2020]. Radiology Cardiothorac Imaging. 10.1148/ryct.2020200422 - DOI - PMC - PubMed
-
- Worldometer . COVID‐19 CORONAVIRUS PANDEMIC; 2021. https://www.worldometers.info/coronavirus/. Accessed February 7, 2021.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
