

Clinical disease activity and flare in SLE: Current concepts and novel biomarkers
- PMID: 33631651
- PMCID: PMC8044029
- DOI: 10.1016/j.jaut.2021.102615
Clinical disease activity and flare in SLE: Current concepts and novel biomarkers
Abstract
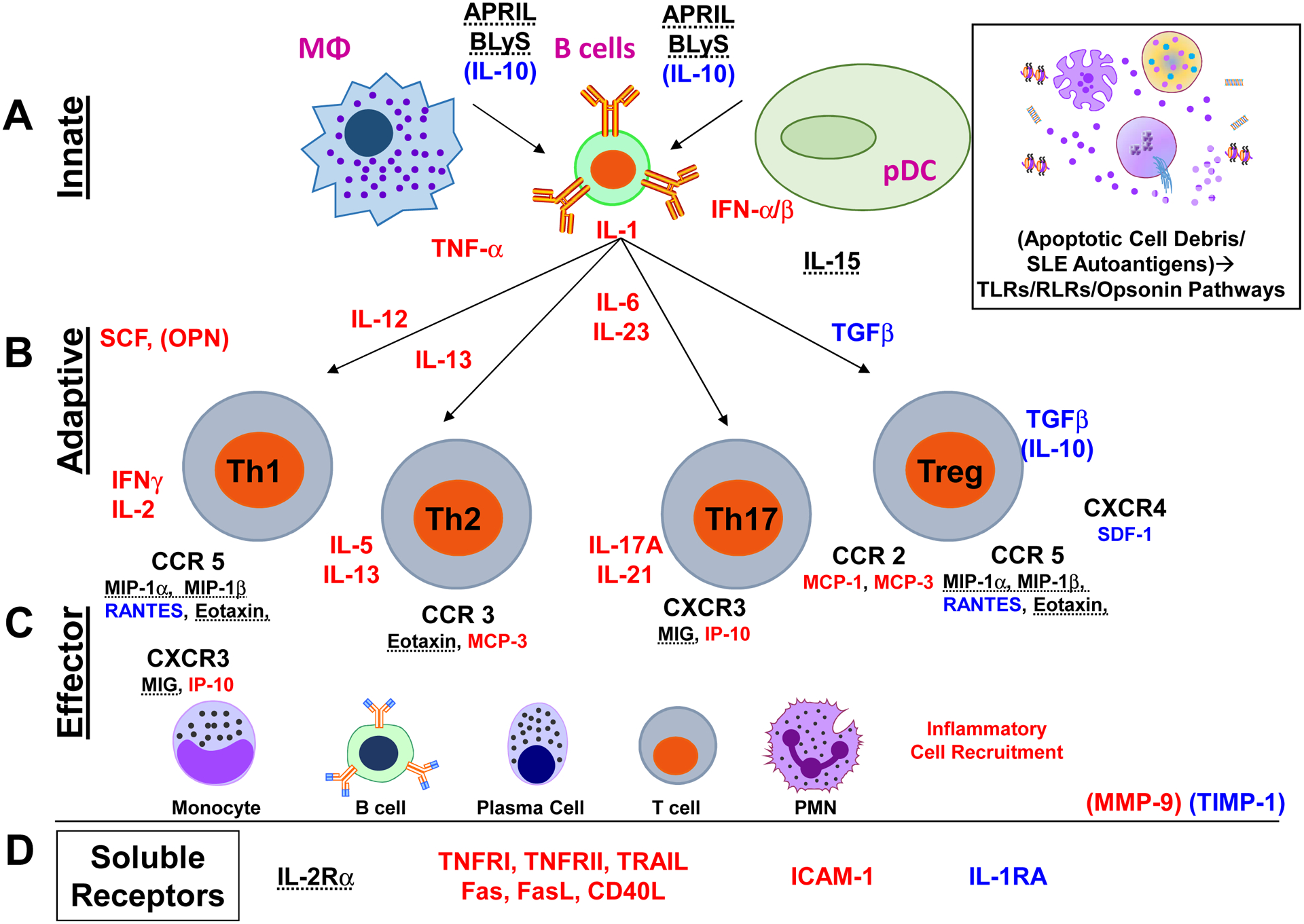
Systemic lupus erythematosus (SLE) is a complex and heterogeneous systemic autoimmune disease associated with innate and adaptive immune dysregulation. SLE occurs primarily in females of childbearing age, with increased prevalence and severity in minority populations. Despite improvements in treatment modalities, SLE patients frequently experience periods of heightened disease activity and flare that can lead to permanent organ damage, increased morbidity, and early mortality. Such outcomes impair quality of life and inflict a significant socioeconomic burden. Predicting changes in SLE disease activity could allow for closer monitoring and preemptive treatment, but existing clinical, demographic and serologic markers have been only modestly predictive. Novel, proactive approaches to clinical disease management are thus critically needed. Panels of blood biomarkers can detect a breadth of immune pathway dysregulation that captures SLE heterogeneity and disease activity. Alterations in the balance of pro-inflammatory and regulatory soluble mediators have been associated with changes in clinical disease activity and are detectable several weeks prior to clinical flare occurrence. A soluble mediator score has been highly predictive of impending flare in both European American and African American SLE patients, and this score does not require a priori knowledge of specific pathway activation in the patient. We review current concepts of disease activity and flare in SLE, focusing on the potential of novel blood biomarkers to characterize and predict changes in disease activity. Measuring the disordered immune response in SLE in this way promises to improve disease management and prevent organ damage in SLE.
Keywords: Biomarkers; Clinical disease activity; Clinical disease flare; Cytokines; Forecasting; Systemic lupus erythematosus.
Copyright © 2021 Progentec Diagnostics, Inc. Published by Elsevier Ltd.. All rights reserved.
Figures

References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
