

Airway gene-expression classifiers for respiratory syncytial virus (RSV) disease severity in infants
- PMID: 33632195
- PMCID: PMC7908785
- DOI: 10.1186/s12920-021-00913-2
Airway gene-expression classifiers for respiratory syncytial virus (RSV) disease severity in infants
Abstract
Background: A substantial number of infants infected with RSV develop severe symptoms requiring hospitalization. We currently lack accurate biomarkers that are associated with severe illness.
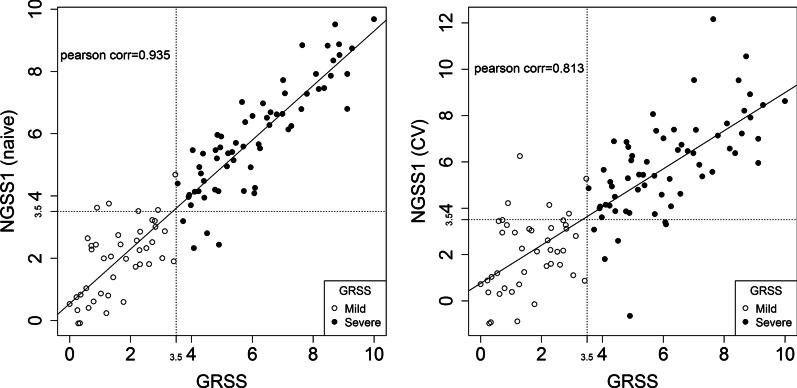
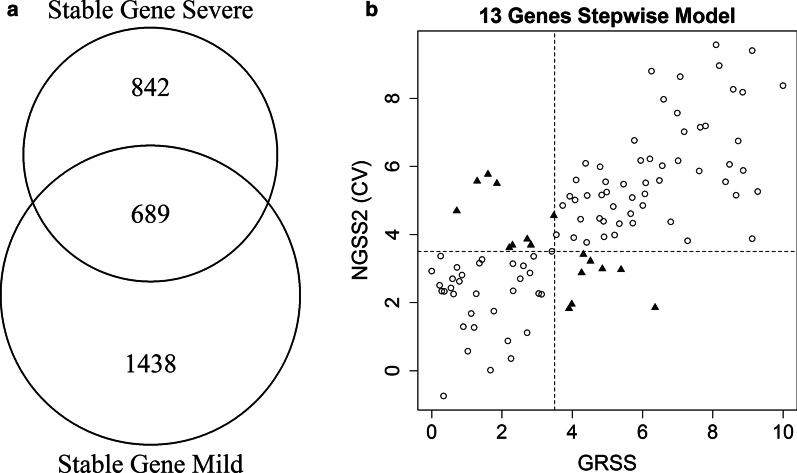
Method: We defined airway gene expression profiles based on RNA sequencing from nasal brush samples from 106 full-tem previously healthy RSV infected subjects during acute infection (day 1-10 of illness) and convalescence stage (day 28 of illness). All subjects were assigned a clinical illness severity score (GRSS). Using AIC-based model selection, we built a sparse linear correlate of GRSS based on 41 genes (NGSS1). We also built an alternate model based upon 13 genes associated with severe infection acutely but displaying stable expression over time (NGSS2).
Results: NGSS1 is strongly correlated with the disease severity, demonstrating a naïve correlation (ρ) of ρ = 0.935 and cross-validated correlation of 0.813. As a binary classifier (mild versus severe), NGSS1 correctly classifies disease severity in 89.6% of the subjects following cross-validation. NGSS2 has slightly less, but comparable, accuracy with a cross-validated correlation of 0.741 and classification accuracy of 84.0%.
Conclusion: Airway gene expression patterns, obtained following a minimally-invasive procedure, have potential utility for development of clinically useful biomarkers that correlate with disease severity in primary RSV infection.
Keywords: Classification; Gene expression; RNA-seq; Respiratory severity score; Respiratory syncytial virus.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
Cilia-related gene signature in the nasal mucosa correlates with disease severity and outcomes in critical respiratory syncytial virus bronchiolitis.Front Immunol. 2022 Sep 23;13:924792. doi: 10.3389/fimmu.2022.924792. eCollection 2022. Front Immunol. 2022. PMID: 36211387 Free PMC article.
-
Airway Gene Expression Correlates of Respiratory Syncytial Virus Disease Severity and Microbiome Composition in Infants.J Infect Dis. 2021 May 20;223(9):1639-1649. doi: 10.1093/infdis/jiaa576. J Infect Dis. 2021. PMID: 32926149 Free PMC article.
-
Differential interferon gene expression in bronchiolitis caused by respiratory syncytial virus-A genotype ON1.Med Microbiol Immunol. 2020 Feb;209(1):23-28. doi: 10.1007/s00430-019-00633-6. Epub 2019 Sep 4. Med Microbiol Immunol. 2020. PMID: 31485724
-
Association of Dynamic Changes in the CD4 T-Cell Transcriptome With Disease Severity During Primary Respiratory Syncytial Virus Infection in Young Infants.J Infect Dis. 2017 Nov 15;216(8):1027-1037. doi: 10.1093/infdis/jix400. J Infect Dis. 2017. PMID: 28962005 Free PMC article.
-
Biomarkers for Disease Severity in Children Infected With Respiratory Syncytial Virus: A Systematic Literature Review.J Infect Dis. 2020 Oct 7;222(Suppl 7):S648-S657. doi: 10.1093/infdis/jiaa208. J Infect Dis. 2020. PMID: 32794555
Cited by
-
Host Subcellular Organelles: Targets of Viral Manipulation.Int J Mol Sci. 2024 Jan 29;25(3):1638. doi: 10.3390/ijms25031638. Int J Mol Sci. 2024. PMID: 38338917 Free PMC article. Review.
-
Cilia-related gene signature in the nasal mucosa correlates with disease severity and outcomes in critical respiratory syncytial virus bronchiolitis.Front Immunol. 2022 Sep 23;13:924792. doi: 10.3389/fimmu.2022.924792. eCollection 2022. Front Immunol. 2022. PMID: 36211387 Free PMC article.
-
A systems genomics approach uncovers molecular associates of RSV severity.PLoS Comput Biol. 2021 Dec 28;17(12):e1009617. doi: 10.1371/journal.pcbi.1009617. eCollection 2021 Dec. PLoS Comput Biol. 2021. PMID: 34962914 Free PMC article.
-
Gene Expression Risk Scores for COVID-19 Illness Severity.bioRxiv [Preprint]. 2021 Aug 24:2021.08.24.457521. doi: 10.1101/2021.08.24.457521. bioRxiv. 2021. Update in: J Infect Dis. 2023 Feb 1;227(3):322-331. doi: 10.1093/infdis/jiab568. PMID: 34462743 Free PMC article. Updated. Preprint.
-
Temporal Dysbiosis of Infant Nasal Microbiota Relative to Respiratory Syncytial Virus Infection.J Infect Dis. 2021 May 20;223(9):1650-1658. doi: 10.1093/infdis/jiaa577. J Infect Dis. 2021. PMID: 32926147 Free PMC article.
References
-
- Shi T, McAllister DA, O'Brien KL, Simoes EAF, Madhi SA, Gessner BD, Polack FP, Balsells E, Acacio S, Aguayo C, et al. Global, regional, and national disease burden estimates of acute lower respiratory infections due to respiratory syncytial virus in young children in 2015: a systematic review and modelling study. Lancet. 2017;390(10098):946–958. doi: 10.1016/S0140-6736(17)30938-8. - DOI - PMC - PubMed
-
- Hall CB, Weinberg GA, Blumkin AK, Edwards KM, Staat MA, Schultz AF, Poehling KA, Szilagyi PG, Griffin MR, Williams JV, et al. Respiratory syncytial virus-associated hospitalizations among children less than 24 months of age. Pediatrics. 2013;132(2):e341–348. doi: 10.1542/peds.2013-0303. - DOI - PubMed
-
- Bekhof J, Reimink R, Brand PL. Systematic review: insufficient validation of clinical scores for the assessment of acute dyspnoea in wheezing children. Paediatr Respir Rev. 2014;15(1):98–112. - PubMed
-
- Corneli HM, Zorc JJ, Holubkov R, Bregstein JS, Brown KM, Mahajan P, Kuppermann N. Bronchiolitis Study Group for the Pediatric Emergency Care Applied Research N: Bronchiolitis: clinical characteristics associated with hospitalization and length of stay. Pediatr Emerg Care. 2012;28(2):99–103. doi: 10.1097/PEC.0b013e3182440b9b. - DOI - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
