

Mutation spectrum of EXT1 and EXT2 in the Saudi patients with hereditary multiple exostoses
- PMID: 33632255
- PMCID: PMC7905910
- DOI: 10.1186/s13023-021-01738-z
Mutation spectrum of EXT1 and EXT2 in the Saudi patients with hereditary multiple exostoses
Abstract
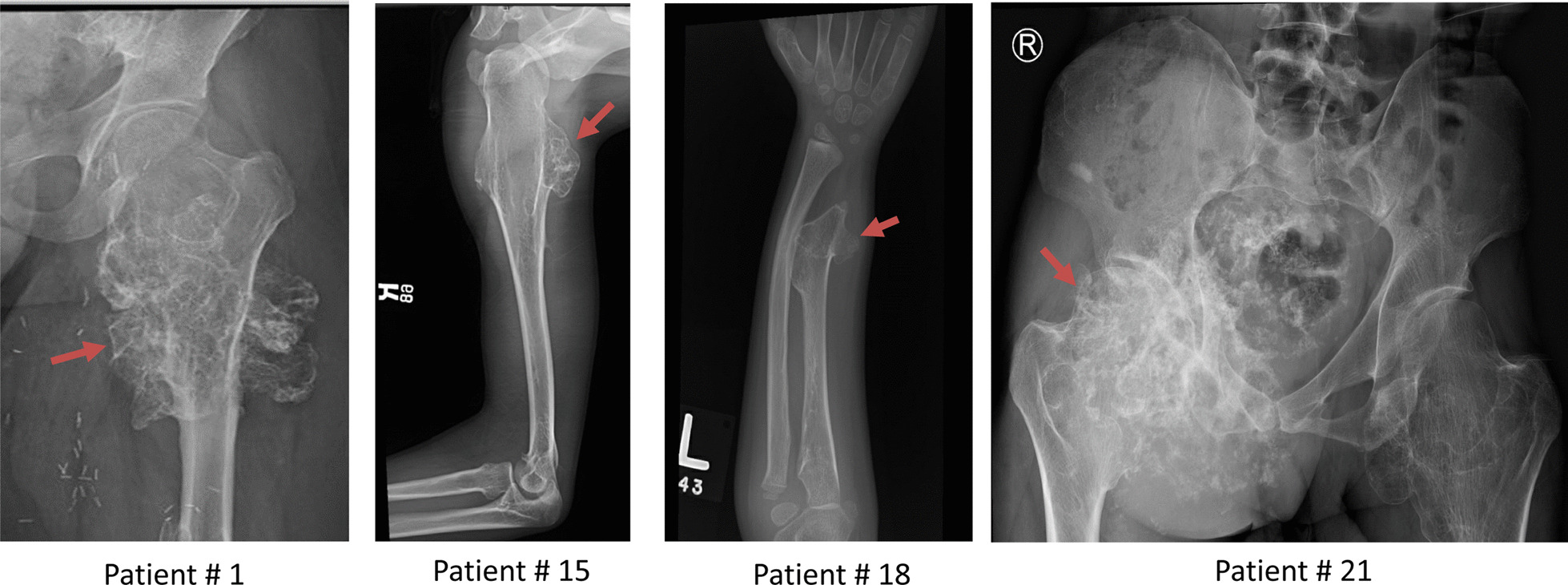
Background: Hereditary Multiple Exostoses (HME), also known as Multiple Osteochondromas (MO) is a rare genetic disorder characterized by multiple benign cartilaginous bone tumors, which are caused by mutations in the genes for exostosin glycosyltransferase 1 (EXT1) and exostosin glycosyltransferase 2 (EXT2). The genetic defects have not been studied in the Saudi patients.
Aim of study: We investigated mutation spectrum of EXT1 and EXT2 in 22 patients from 17 unrelated families.
Methods: Genomic DNA was extracted from peripheral leucocytes. The coding regions and intron-exon boundaries of both EXT1 and EXT2 genes were screened for mutations by PCR-sequencing analysis. Gross deletions were analyzed by MLPA analysis.
Results: EXT1 mutations were detected in 6 families (35%) and 3 were novel mutations: c.739G > T (p. E247*), c.1319delG (p.R440Lfs*4), and c.1786delA (p.S596Afs*25). EXT2 mutations were detected in 7 families (41%) and 3 were novel mutations: c.541delG (p.D181Ifs*89), c.583delG (p.G195Vfs*75), and a gross deletion of approximately 10 kb including promoter and exon 1. Five patients from different families had no family history and carried de novo mutations (29%, 5/17). No EXT1 and EXT2 mutations were found in the remaining four families. In total, EXT1 and EXT2 mutations were found in 77% (13/17) of Saudi HME patients.
Conclusion: EXT1 and EXT2 mutations contribute significantly to the pathogenesis of HME in the Saudi population. In contrast to high mutation rate in EXT 1 (65%) and low mutation rate in EXT2 (25%) in other populations, the frequency of EXT2 mutations are much higher (41%) and comparable to that of EXT1 among Saudi patients. De novo mutations are also common and the six novel EXT1/EXT2 mutations further expands the mutation spectrum of HME.
Keywords: EXT1; EXT12; Exostoses; Mutation; Osteochondromas.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures


References
-
- Jennes I, Pedrini E, Zuntini M, Mordenti M, Balkassmi S, Asteggiano CG, Casey B, Bakker B, Sangiorgi L, Wuyts W. Multiple osteochondromas: mutation update and description of the multiple osteochondromas mutation database (MOdb) Hum Mutat. 2009;30(12):1620–1627. doi: 10.1002/humu.21123. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
