

Timeout procedure in paediatric surgery: effective tool or lip service? A randomised prospective observational study
- PMID: 33632757
- PMCID: PMC8311082
- DOI: 10.1136/bmjqs-2020-012001
Timeout procedure in paediatric surgery: effective tool or lip service? A randomised prospective observational study
Abstract
Background: For over a decade, the preoperative timeout procedure has been implemented in most paediatric surgery units. However, the impact of this intervention has not been systematically studied. This study evaluates whether purposefully introduced errors during the timeout routine are detected and reported by the operating team members.
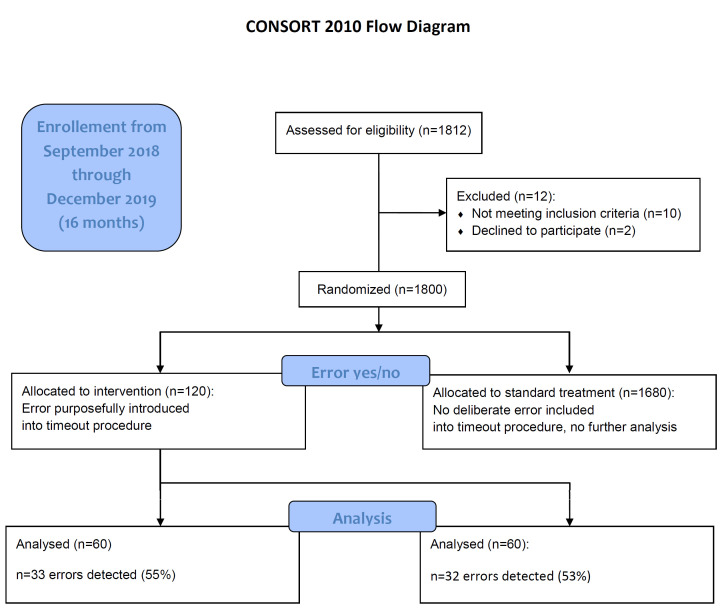
Methods: After ethics board approval and informed consent, deliberate errors were randomly and clandestinely introduced into the timeout routine for elective surgical procedures by a paediatric surgery attending. Errors were randomly selected among wrong name, site, side, allergy, intervention, birthdate and gender items. The main outcome measure was how frequent an error was reported by the team and by whom.
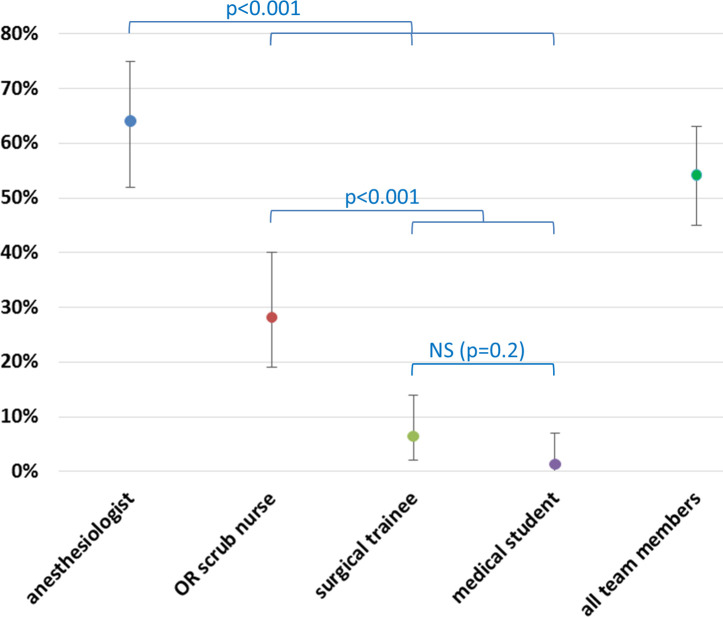
Results: Over the course of 16 months, 1800 operations and timeouts were performed. Errors were randomly introduced in 120 cases (6.7%). Overall, 54% of the errors were reported; the remainder went unnoticed. Errors were pointed out most frequently by anaesthesiologists (64%), followed by nursing staff (28%), residents-in-training (6%) and medical students (1%).
Conclusion: Errors in the timeout routine go unnoticed by the team in almost half of cases. Therefore, even if preoperative timeout routines are strictly implemented, mistakes may be overlooked. Hence, the timeout procedure in its current form appears unreliable. Future developments may be useful to improve the quality of the surgical timeout and should be studied in detail.
Keywords: Paediatrics; human error; measurement/epidemiology; medical error; safety culture; surgery.
© Author(s) (or their employer(s)) 2021. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
Comment in
-
Time out! Rethinking surgical safety: more than just a checklist.BMJ Qual Saf. 2021 Aug;30(8):613-617. doi: 10.1136/bmjqs-2020-012600. Epub 2021 Mar 23. BMJ Qual Saf. 2021. PMID: 33758034 No abstract available.
-
Surgical safety checklist: fact or fake?Einstein (Sao Paulo). 2022 Sep 12;20:eCE0059. doi: 10.31744/einstein_journal/2022CE0059. eCollection 2022. Einstein (Sao Paulo). 2022. PMID: 36102408 Free PMC article. No abstract available.
Similar articles
-
Clinical risk management - a 3-year experience of team timeout in 18 081 ophthalmic patients.Acta Ophthalmol. 2017 Mar;95(2):e89-e94. doi: 10.1111/aos.13155. Epub 2016 Jul 16. Acta Ophthalmol. 2017. PMID: 27422210
-
No signs of check-list fatigue - introducing the StOP? intra-operative briefing enhances the quality of an established pre-operative briefing in a pre-post intervention study.Front Psychol. 2023 Jun 29;14:1195024. doi: 10.3389/fpsyg.2023.1195024. eCollection 2023. Front Psychol. 2023. PMID: 37457099 Free PMC article.
-
Implementation of an Intraoperative Instructional Timeout Just Prior to Stapler Use Improves Proficiency of Surgical Stapler Usage by Surgery Residents.J Surg Educ. 2019 Nov-Dec;76(6):1622-1628. doi: 10.1016/j.jsurg.2019.05.005. Epub 2019 Jun 22. J Surg Educ. 2019. PMID: 31239232
-
Effectiveness of the surgical safety checklist in correcting errors: a literature review applying Reason's Swiss cheese model.AORN J. 2014 Jul;100(1):65-79.e5. doi: 10.1016/j.aorn.2013.07.024. AORN J. 2014. PMID: 24973186 Review.
-
Ensuring correct site surgery.AORN J. 2002 Nov;76(5):770-7; quiz 779-82. doi: 10.1016/s0001-2092(06)61029-6. AORN J. 2002. PMID: 12463077 Review.
Cited by
-
Compliance with the surgical safety checklist in Switzerland: an observational multicenter study based on self-reported data.Patient Saf Surg. 2022 May 25;16(1):17. doi: 10.1186/s13037-022-00327-8. Patient Saf Surg. 2022. PMID: 35614454 Free PMC article.
-
Healthcare professionals' perception of the World Health Organization Surgical Safety Checklist and psychological safety: a cross-sectional survey.BMJ Open Qual. 2024 Dec 9;13(4):e003154. doi: 10.1136/bmjoq-2024-003154. BMJ Open Qual. 2024. PMID: 39653512 Free PMC article.
-
Surgical safety checklist: fact or fake?Einstein (Sao Paulo). 2022 Sep 12;20:eCE0059. doi: 10.31744/einstein_journal/2022CE0059. eCollection 2022. Einstein (Sao Paulo). 2022. PMID: 36102408 Free PMC article. No abstract available.
-
[User behavior during functional testing of the ventilator: analysis of the use of the QUICKcheck and detection of misconnected ventilation tubes].Anaesthesiologie. 2025 Feb;74(2):72-80. doi: 10.1007/s00101-024-01496-0. Epub 2025 Jan 30. Anaesthesiologie. 2025. PMID: 39884980 Free PMC article. German.
References
-
- WHO . Safe surgery: World Health Organization, 2008. Available: http://who.int/patientsafety/safesurgery/en/ [Accessed 11 Mar 2020].
-
- Degani A, Wiener EL. Cockpit checklists: concepts, design, and use. Hum Factors 1993;35:345–59. 10.1177/001872089303500209 - DOI
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical