

Development and validation of a prediction model for 30-day mortality in hospitalised patients with COVID-19: the COVID-19 SEIMC score
- PMID: 33632764
- PMCID: PMC7908055
- DOI: 10.1136/thoraxjnl-2020-216001
Development and validation of a prediction model for 30-day mortality in hospitalised patients with COVID-19: the COVID-19 SEIMC score
Abstract
Objective: To develop and validate a prediction model of mortality in patients with COVID-19 attending hospital emergency rooms.
Design: Multivariable prognostic prediction model.
Setting: 127 Spanish hospitals.
Participants: Derivation (DC) and external validation (VC) cohorts were obtained from multicentre and single-centre databases, including 4035 and 2126 patients with confirmed COVID-19, respectively.
Interventions: Prognostic variables were identified using multivariable logistic regression.
Main outcome measures: 30-day mortality.
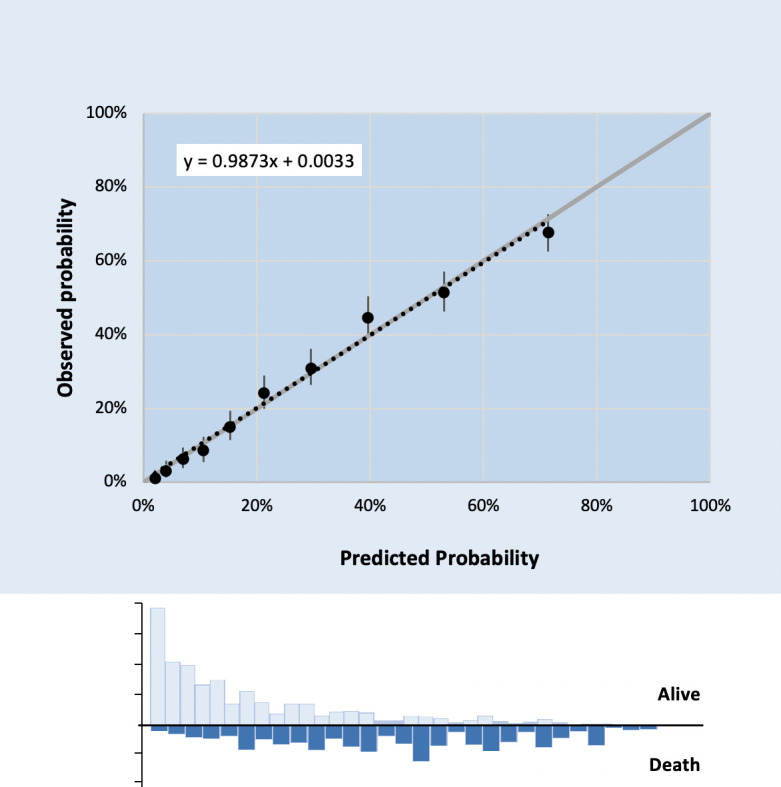
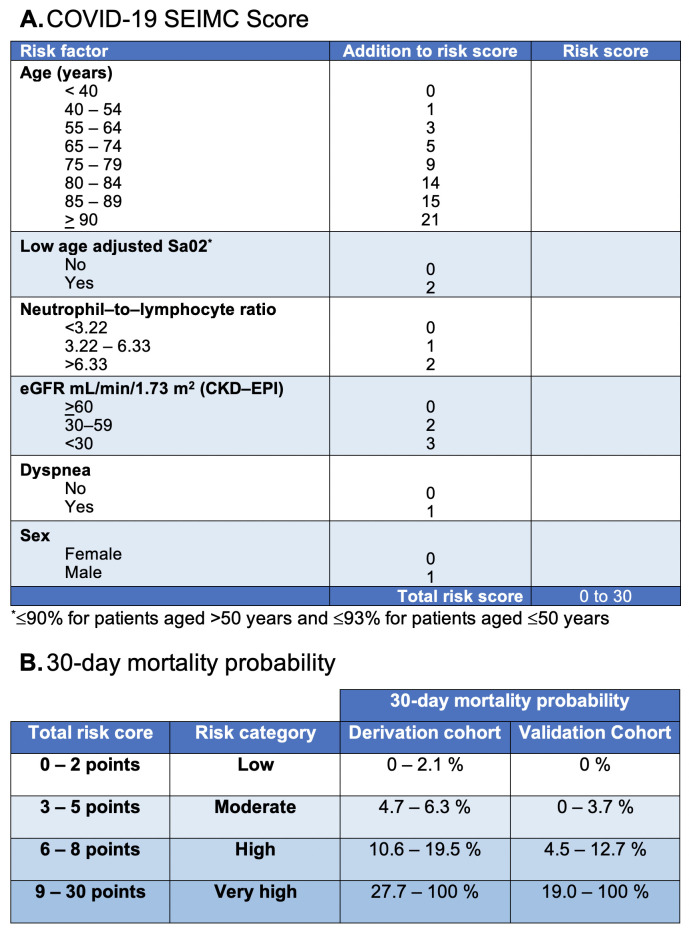
Results: Patients' characteristics in the DC and VC were median age 70 and 61 years, male sex 61.0% and 47.9%, median time from onset of symptoms to admission 5 and 8 days, and 30-day mortality 26.6% and 15.5%, respectively. Age, low age-adjusted saturation of oxygen, neutrophil-to-lymphocyte ratio, estimated glomerular filtration rate by the Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) equation, dyspnoea and sex were the strongest predictors of mortality. Calibration and discrimination were satisfactory with an area under the receiver operating characteristic curve with a 95% CI for prediction of 30-day mortality of 0.822 (0.806-0.837) in the DC and 0.845 (0.819-0.870) in the VC. A simplified score system ranging from 0 to 30 to predict 30-day mortality was also developed. The risk was considered to be low with 0-2 points (0%-2.1%), moderate with 3-5 (4.7%-6.3%), high with 6-8 (10.6%-19.5%) and very high with 9-30 (27.7%-100%).
Conclusions: A simple prediction score, based on readily available clinical and laboratory data, provides a useful tool to predict 30-day mortality probability with a high degree of accuracy among hospitalised patients with COVID-19.
Keywords: clinical epidemiology; critical care; emergency medicine; pneumonia; respiratory infection; viral infection.
© Author(s) (or their employer(s)) 2021. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: JB reports grants and personal fees from GILEAD, MSD and ViiV Healthcare; and personal fees from JANSSEN, outside the submitted work. PR reports grants and personal fees from GILEAD and MSD; and personal fees from AbbVie and ViiV Healthcare, outside the submitted work. IJ reports personal fees from GILEAD and ViiV Healthcare, outside the submitted work. JRA reports grants and personal fees from GILEAD and ViiV Healthcare; and personal fees from ALEXA, MSD, JANSSEN, SERONO and TEVA, outside the submitted work. The remaining authors have nothing to disclose.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical