

Radiological dynamics and SITC-defined resistance types of advanced melanoma during anti-PD-1 monotherapy: an independent single-blind observational study on an international cohort
- PMID: 33632901
- PMCID: PMC7908917
- DOI: 10.1136/jitc-2020-002092
Radiological dynamics and SITC-defined resistance types of advanced melanoma during anti-PD-1 monotherapy: an independent single-blind observational study on an international cohort
Abstract
Background: Although the Society for Immunotherapy of Cancer (SITC) Immunotherapy Resistance Taskforce recently defined primary and secondary resistance to anti-programmed cell death protein 1 (anti-PD-1) therapy, there is lack of real-world data regarding differences in these resistance subtypes with respect to radiological dynamics and clinical manifestations.
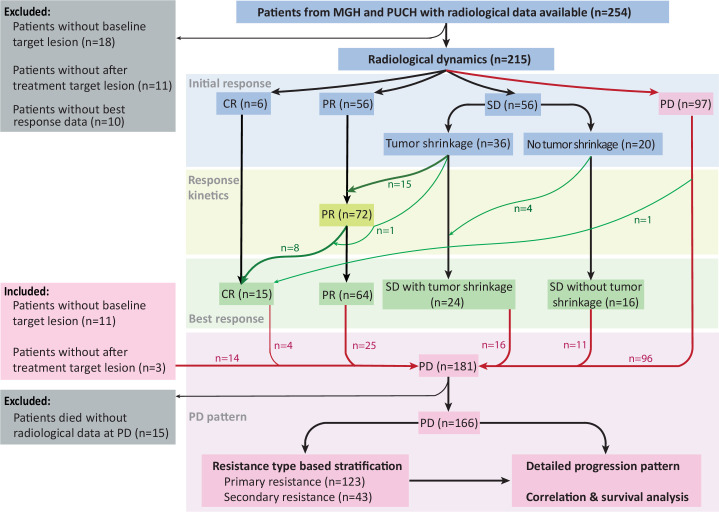
Methods: We performed single-blind re-evaluations of radiological images by independent radiologists on a retrospectively assembled cohort of patients with advanced melanoma (n=254, median follow-up 31 months) receiving anti-PD-1 monotherapy at Massachusetts General Hospital and Peking University Cancer Hospital. Radiological characteristics and timing at multiple crucial time points were analyzed and correlated with each other and with survival. Primary and secondary resistance was defined as per the SITC Immunotherapy Resistance Taskforce definitions.
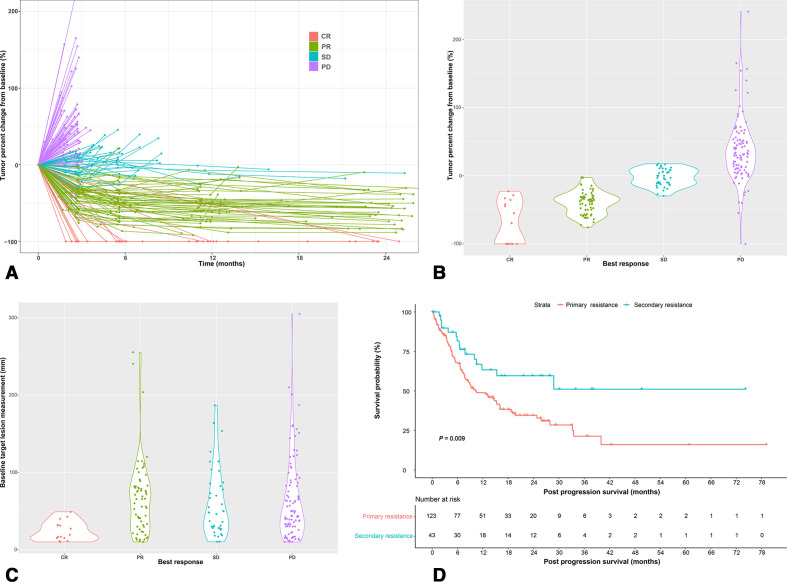
Results: The most significant target lesion measurement change took place within the first 3 months after anti-PD-1 initiation. Patients with stable disease with versus without tumor shrinkage at the initial evaluation exhibited distinct disease trajectory, as the rate of further upgrade to a partial or complete remission (CR/PR) was 44% and 0%, respectively. Eleven per cent of PR patients ultimately achieved a CR. In multivariate analyses, deeper response depth was independently associated with a more limited progression pattern, fewer involved organs, lower tumor burden, slower growth rate at disease progression (PD) (all p≤0.001), and longer post-progression survival (PPS) (bivariate analysis, p=0.005). Compared with primary resistance, secondary resistance was associated with less widespread PD pattern, lower tumor burden and slower tumor growth (all p≤0.001). Patients with secondary resistance were less likely to receive further systemic therapy (28% vs 57%, p<0.001) yet had significantly better PPS (HR 0.503, 95% CI 0.288 to 0.879, p=0.02).
Conclusions: Radiological dynamics were variable, yet significantly correlated with survival outcomes. SITC-defined primary and secondary resistance are distinct clinical manifestations in patients with melanoma, suggesting the possibility of resistance-type-based therapeutic decision-making and clinical trial design, once further validated by future prospective studies.
Keywords: immunotherapy; melanoma; programmed cell death 1 receptor.
© Author(s) (or their employer(s)) 2021. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: Dr XB receives a merit award supported by BMS. Dr JC serves as a consultant for BMS and Sanofi-Genzyme. KR serves on advisory boards for Merck & BMS. Dr KF serves on the Board of Directors of Loxo Oncology, Clovis Oncology, Strata Oncology and Vivid Biosciences; on the Corporate Advisory Boards of X4 Pharmaceuticals and PIC Therapeutics; on the scientific advisory boards of Sanofi, Amgen, Asana, Adaptimmune, Fount, Aeglea, Array BioPharma, Shattuck Labs, Arch Oncology, Tolero, Apricity, Oncoceutics, Fog Pharma, Neon Therapeutics and Tvardi; and as a consultant to Novartis, Genentech, BMS, Merck, Takeda, Verastem, Checkmate, Boston Biomedical, Pierre Fabre, Cell Medica and Debiopharm. Dr RS serves as consultant for Amgen, Asana Biosciences, BMS, Merck, Novartis, Array BioPharma, Compugen, and Replimune; he receives research support from Amgen and Merck. Dr JG serves as consultant or is on advisory boards for MSD, Roche, Pfizer, Bayer, Novartis, Simcere Pharmaceutical Group, Shanghai Junshi Biosciences, and Oriengene. Dr GB has a sponsored research agreement with Takeda Oncology, Olink Proteomics, and Palleon Pharmaceuticals; serves as a consultant for NW Biotherapeutics, served as a speaker for Novartis and Takeda Oncology; and served on a scientific advisory board and steering committee for Nektar Therapeutics. All remaining authors have declared no conflicts of interest.
Figures
References
-
- Osgood C, Mulkey F, Mishra-Kalyani PS, et al. FDA analysis of depth of response (Dpr) and survival across 10 randomized controlled trials in patients with previously untreated unresectable or metastatic melanoma (Umm) by therapy type. J Clin Oncol 2019;37:9508. 10.1200/JCO.2019.37.15_suppl.9508 - DOI
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials