

Phenobarbital and Clonidine as Secondary Medications for Neonatal Opioid Withdrawal Syndrome
- PMID: 33632932
- PMCID: PMC7919109
- DOI: 10.1542/peds.2020-017830
Phenobarbital and Clonidine as Secondary Medications for Neonatal Opioid Withdrawal Syndrome
Abstract
Background and objectives: Despite the neonatal opioid withdrawal syndrome (NOWS) epidemic in the United States, evidence is limited for pharmacologic management when first-line opioid medications fail to control symptoms. The objective with this study was to evaluate outcomes of infants receiving secondary therapy with phenobarbital compared with clonidine, in combination with morphine, for the treatment of NOWS.
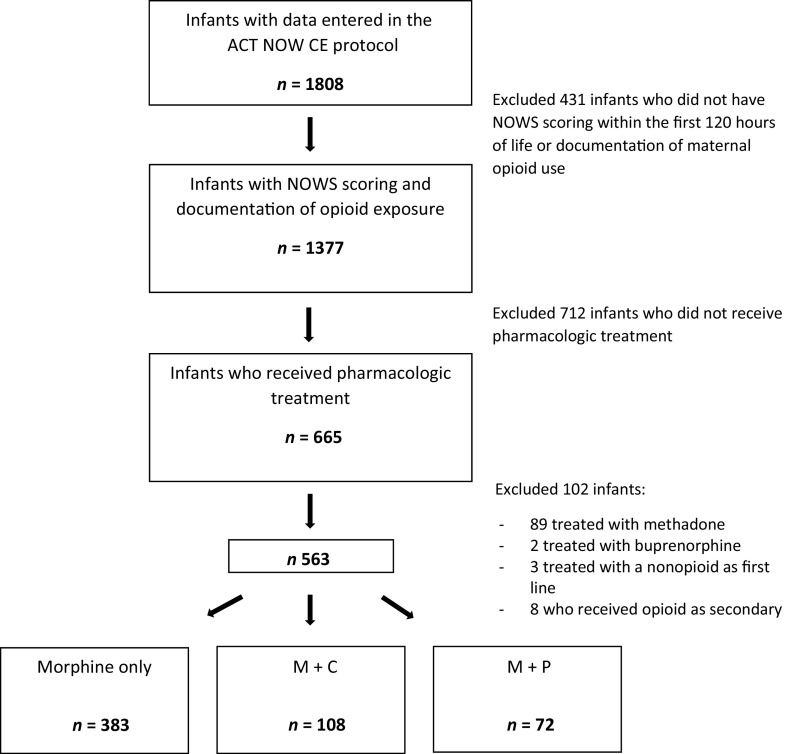
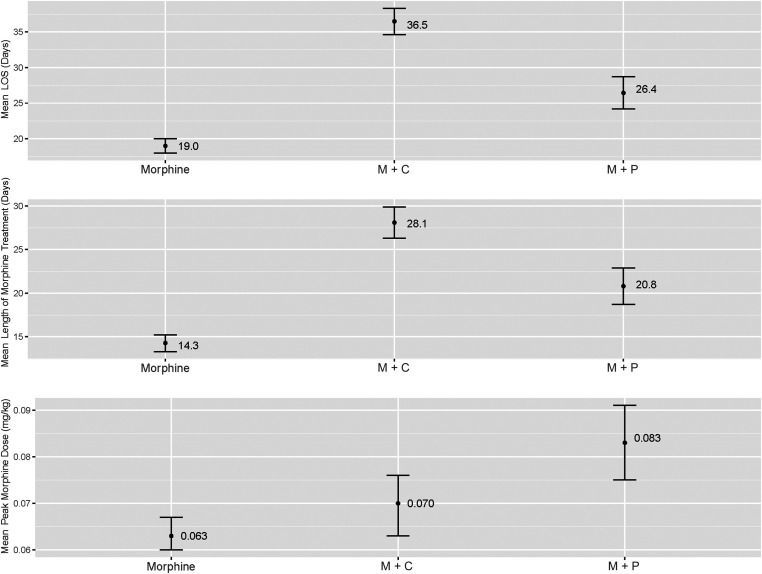
Methods: We performed a retrospective cohort study of infants with NOWS from 30 hospitals. The primary outcome measures were the length of hospital stay, duration of opioid treatment, and peak morphine dose. Outcomes were compared by group by using analysis of variance and multivariable linear regression controlling for relevant confounders.
Results: Of 563 infants with NOWS treated with morphine, 32% (n = 180) also received a secondary medication. Seventy-two received phenobarbital and 108 received clonidine. After adjustment for covariates, length of hospital stay was 10 days shorter, and, in some models, duration of morphine treatment was 7.5 days shorter in infants receiving phenobarbital compared with those receiving clonidine, with no difference in peak morphine dose. Infants were more likely to be discharged from the hospital on phenobarbital than clonidine (78% vs 29%, P < .0001).
Conclusions: Among infants with NOWS receiving morphine and secondary therapy, those treated with phenobarbital had shorter length of hospital stay and shorter morphine treatment duration than clonidine-treated infants but were discharged from the hospital more often on secondary medication. Further investigation is warranted to determine if the benefits of shorter hospital stay and shorter duration of morphine therapy justify the possible neurodevelopmental consequences of phenobarbital use in infants with NOWS.
Copyright © 2021 by the American Academy of Pediatrics.
Conflict of interest statement
POTENTIAL CONFLICT OF INTEREST: Dr Whalen is a codeveloper of the ESC Care Tool; Children’s Hospital at Dartmouth-Hitchcock is one of the institutions on the ESC Care Tool copyright; the other authors have indicated they have no potential conflicts of interest to disclose.
Figures
Similar articles
-
Buprenorphine vs. morphine: impact on neonatal opioid withdrawal syndrome (NOWS) outcomes in a single center retrospective study.J Perinatol. 2025 Apr;45(4):473-479. doi: 10.1038/s41372-024-02046-7. Epub 2024 Jul 13. J Perinatol. 2025. PMID: 39003405 Free PMC article.
-
Clonidine versus phenobarbital as adjunctive therapy for neonatal abstinence syndrome.J Perinatol. 2020 Jul;40(7):1050-1055. doi: 10.1038/s41372-020-0685-2. Epub 2020 May 18. J Perinatol. 2020. PMID: 32424335
-
Efficacy of clonidine versus phenobarbital in reducing neonatal morphine sulfate therapy days for neonatal abstinence syndrome. A prospective randomized clinical trial.J Perinatol. 2013 Dec;33(12):954-9. doi: 10.1038/jp.2013.95. Epub 2013 Aug 15. J Perinatol. 2013. PMID: 23949834 Clinical Trial.
-
Sedatives for opioid withdrawal in newborn infants.Cochrane Database Syst Rev. 2021 May 18;5(5):CD002053. doi: 10.1002/14651858.CD002053.pub4. Cochrane Database Syst Rev. 2021. PMID: 34002380 Free PMC article.
-
Pharmacotherapy for Neonatal Abstinence Syndrome: Choosing the Right Opioid or No Opioid at All.Neonatal Netw. 2016;35(5):314-20. doi: 10.1891/0730-0832.35.5.314. Neonatal Netw. 2016. PMID: 27636696 Review.
Cited by
-
Use of Phenobarbital to Treat Neonatal Abstinence Syndrome From Exposure to Single vs. Multiple Substances.Front Pediatr. 2022 Jan 31;9:752854. doi: 10.3389/fped.2021.752854. eCollection 2021. Front Pediatr. 2022. PMID: 35174112 Free PMC article.
-
Future Newborns with Opioid-Induced Neonatal Abstinence Syndrome (NAS) Could Be Assessed with the Genetic Addiction Risk Severity (GARS) Test and Potentially Treated Using Precision Amino-Acid Enkephalinase Inhibition Therapy (KB220) as a Frontline Modality Instead of Potent Opioids.J Pers Med. 2022 Dec 6;12(12):2015. doi: 10.3390/jpm12122015. J Pers Med. 2022. PMID: 36556236 Free PMC article. Review.
-
Comparison of Two Morphine Dosing Strategies in the Management of Neonatal Abstinence Syndrome.J Pediatr Pharmacol Ther. 2022;27(2):151-156. doi: 10.5863/1551-6776-27.2.151. Epub 2022 Feb 9. J Pediatr Pharmacol Ther. 2022. PMID: 35241987 Free PMC article.
-
Neonatal Abstinence Syndrome: A Review of Treatment in the Neonatal Intensive Care Unit.Can J Hosp Pharm. 2023 Jul 5;76(3):234-238. doi: 10.4212/cjhp.3381. eCollection 2023 Summer. Can J Hosp Pharm. 2023. PMID: 37409149 Free PMC article.
-
Optimal Drug, Optimal Dose, or Both in the Pharmacological Treatment of Neonatal Opioid Withdrawal Syndrome?Clin Pharmacol Ther. 2025 May;117(5):1182-1184. doi: 10.1002/cpt.3600. Epub 2025 Feb 11. Clin Pharmacol Ther. 2025. PMID: 39935314 Free PMC article. No abstract available.
References
-
- Hudak ML, Tan RC; Committee on Drugs; Committee on Fetus and Newborn; American Academy of Pediatrics . Neonatal drug withdrawal. Pediatrics. 2012;129(2). Available at: www.pediatrics.org/cgi/content/full/129/2/e540 - PubMed
-
- Sarkar S, Donn SM. Management of neonatal abstinence syndrome in neonatal intensive care units: a national survey. J Perinatol. 2006;26(1):15–17 - PubMed
-
- Hall ES, Wexelblatt SL, Crowley M, et al. .; OCHNAS Consortium . A multicenter cohort study of treatments and hospital outcomes in neonatal abstinence syndrome. Pediatrics. 2014;134(2). Available at: www.pediatrics.org/cgi/content/full/134/2/e527 - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- UG1 OD024945/OD/NIH HHS/United States
- U2C OD023375/OD/NIH HHS/United States
- UG1 OD024943/OD/NIH HHS/United States
- UG1 HD027853/HD/NICHD NIH HHS/United States
- UG1 OD024947/OD/NIH HHS/United States
- UG1 OD024958/OD/NIH HHS/United States
- UG1 HD090907/HD/NICHD NIH HHS/United States
- UG1 OD024946/OD/NIH HHS/United States
- U10 HD036790/HD/NICHD NIH HHS/United States
- UG1 HD068278/HD/NICHD NIH HHS/United States
- UG1 OD024953/OD/NIH HHS/United States
- UG1 OD024950/OD/NIH HHS/United States
- UG1 OD024952/OD/NIH HHS/United States
- U10 HD027904/HD/NICHD NIH HHS/United States
- UG1 OD024951/OD/NIH HHS/United States
- UG1 OD024948/OD/NIH HHS/United States
- UG1 OD024959/OD/NIH HHS/United States
- UG1 HD090875/HD/NICHD NIH HHS/United States
- UG1 OD024942/OD/NIH HHS/United States
- U24 OD024957/OD/NIH HHS/United States
- UG1 OD024954/OD/NIH HHS/United States
- UG1 OD024944/OD/NIH HHS/United States
- UG1 HD021364/HD/NICHD NIH HHS/United States
- UG1 OD024956/OD/NIH HHS/United States
- UG1 OD024949/OD/NIH HHS/United States
- UG1 OD024955/OD/NIH HHS/United States
- U10 HD053089/HD/NICHD NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
