

Reappraisal of the incidence, various types and risk factors of malignancies in patients with dermatomyositis and polymyositis in Taiwan
- PMID: 33633147
- PMCID: PMC7907377
- DOI: 10.1038/s41598-021-83729-5
Reappraisal of the incidence, various types and risk factors of malignancies in patients with dermatomyositis and polymyositis in Taiwan
Abstract
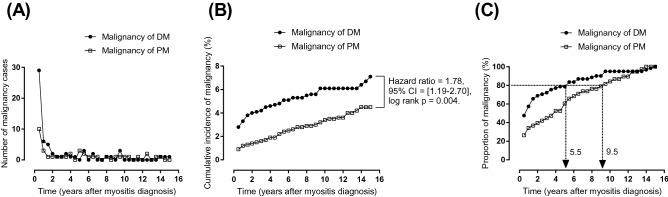
Our study aimed to investigate the incidence, risk factors and time to occurrence of malignancy in patients with dermatomyositis (DM) and polymyositis (PM). The electronic medical records of 1100 patients with DM and 1164 patients with PM were studied between January 2001 and May 2019. Malignancies after myositis were diagnosed in 61 (5.55%) patients with DM and 38 (3.26%) patients with PM. The cumulative incidence of malignancies in patients with DM were significantly higher than patients with PM (hazard ratio = 1.78, log-rank p = 0.004). Patients with DM had a greater risk of developing malignancy than those with PM at 40-59 years old (p = 0.01). Most malignancies occurred within 1 year after the initial diagnosis of DM (n = 35; 57.38%). Nasopharyngeal cancer (NPC) was the most common type of malignancy in patients with DM (22.95%), followed by lung, and breast cancers. In patients with PM, colorectal, lung and hepatic malignancies were the top three types of malignancy. The risk factors for malignancy included old age (≥ 45 years old) and low serum levels of creatine phosphokinase (CPK) for patients with DM and male sex and low serum levels of CPK for patients with PM. Low serum levels of CPK in patients with myositis with malignancy represented a low degree of muscle destruction/inflammation, which might be attributed to activation of the PD-L1 pathway by tumor cells, thus inducing T-cell dysfunction mediating immune responses in myofibers. A treatment and follow-up algorithm should explore the occurrence of malignancy in different tissues and organs and suggested annual follow-ups for at least 5.5 years to cover the 80% cumulative incidence of malignancy in patients with DM and PM.
Conflict of interest statement
The authors declare no competing interests.
Figures

References
-
- Smoyer-Tomic KE, Amato AA, Fernandes AW. Incidence and prevalence of idiopathic inflammatory myopathies among commercially insured, Medicare supplemental insured, and Medicaid enrolled populations: An administrative claims analysis. BMC Musculoskelet. Disord. 2012;13:103. doi: 10.1186/1471-2474-13-103. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
