

Real-time observation of microcirculatory leukocytes in patients undergoing major liver resection
- PMID: 33633168
- PMCID: PMC7907405
- DOI: 10.1038/s41598-021-83677-0
Real-time observation of microcirculatory leukocytes in patients undergoing major liver resection
Abstract
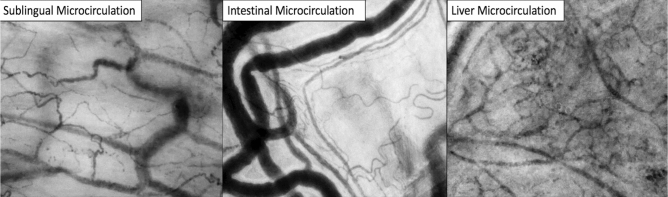
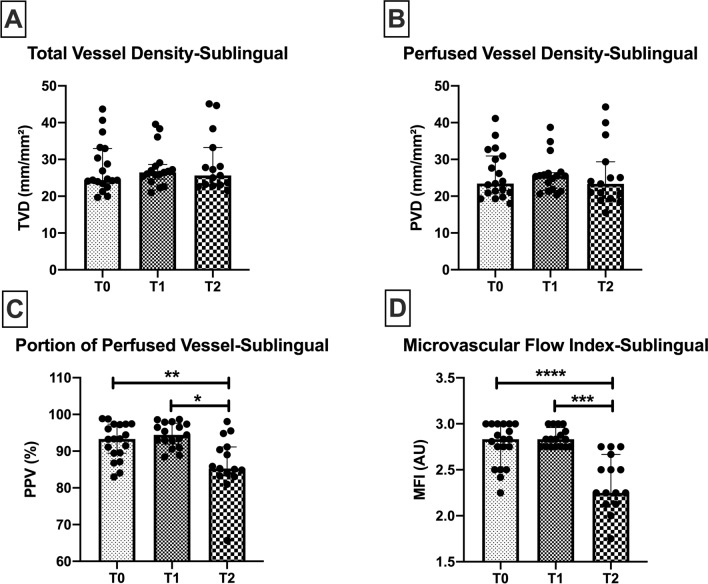
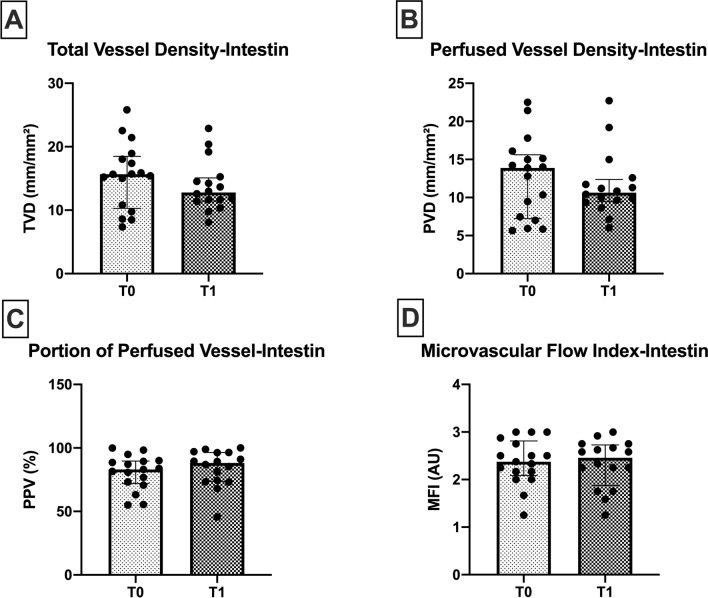
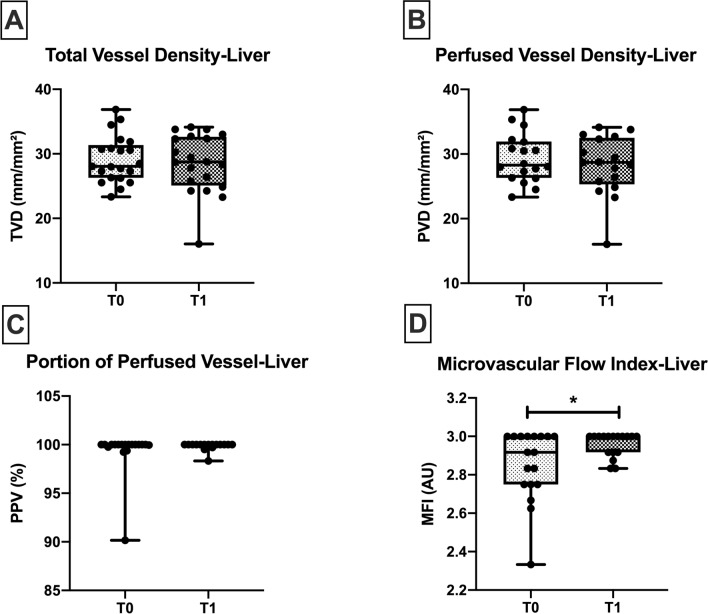
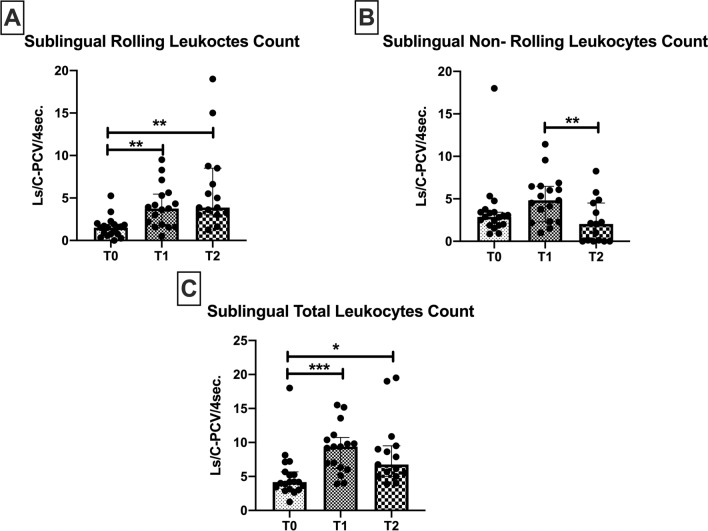
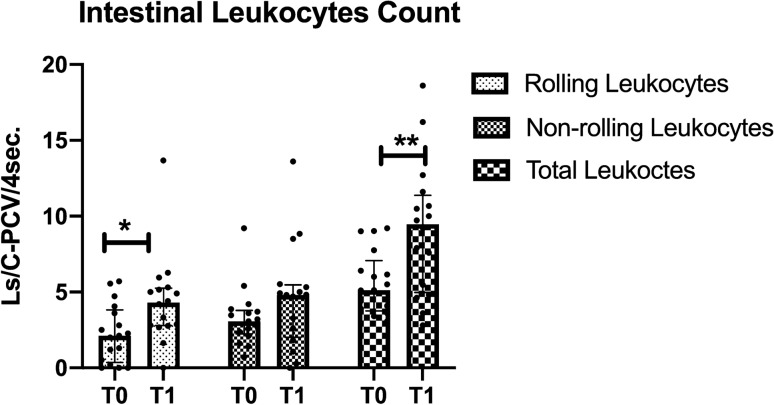
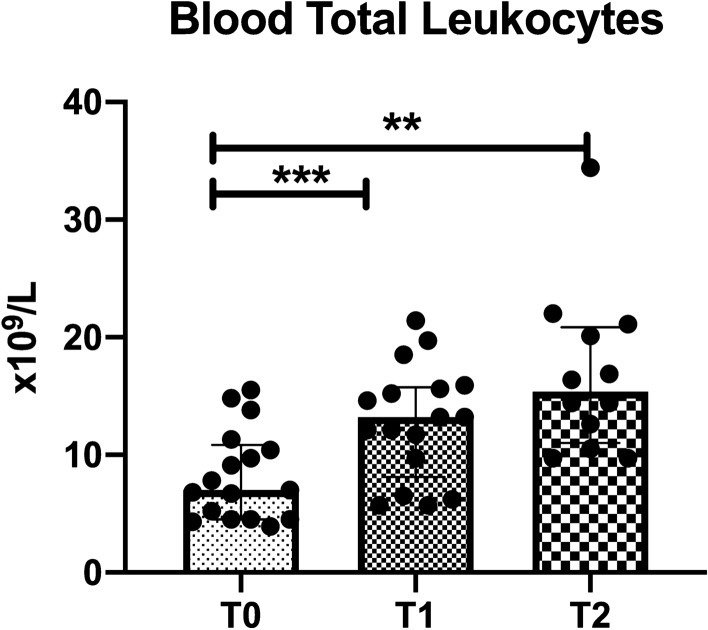
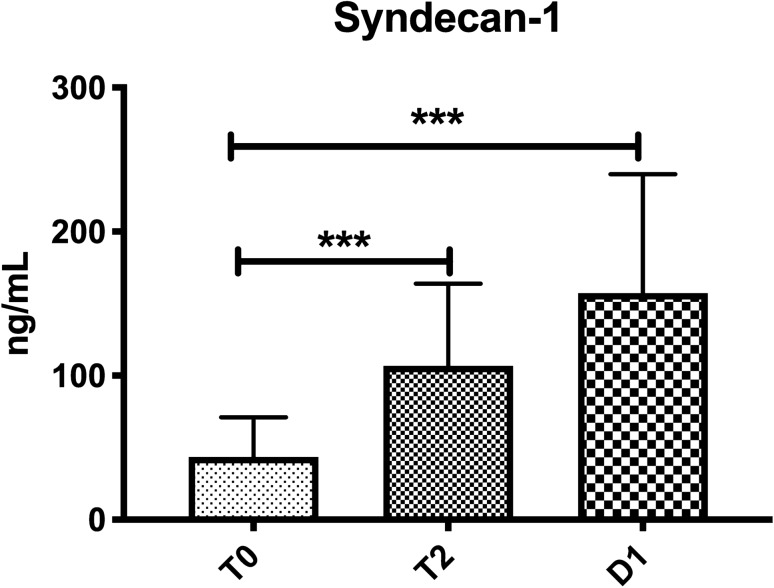
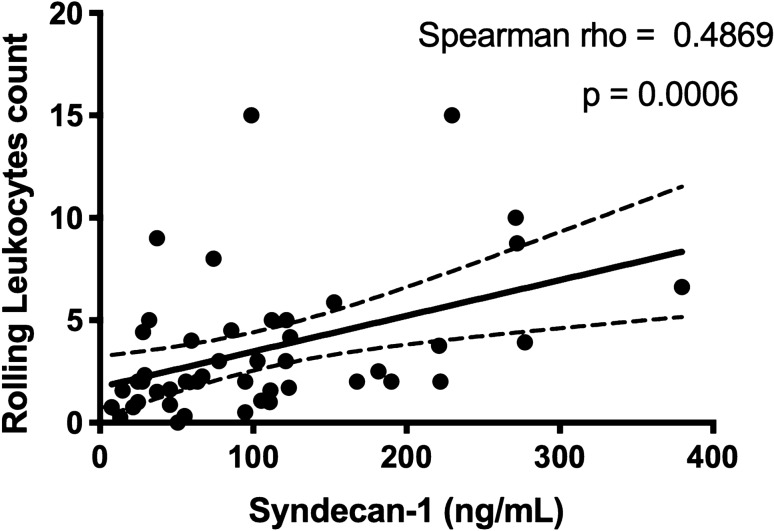
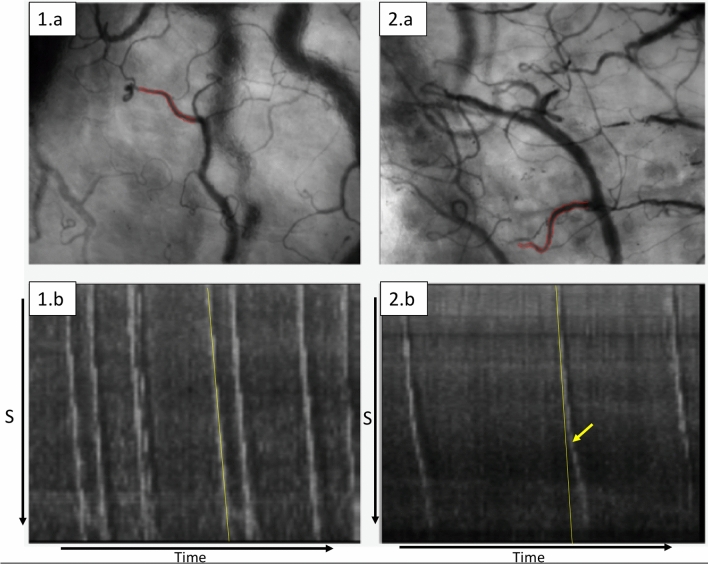
Ischemia/reperfusion injury and inflammation are associated with microcirculatory dysfunction, endothelial injury and glycocalyx degradation. This study aimed to assess microcirculation in the sublingual, intestinal and the (remnant) liver in patients undergoing major liver resection, to define microcirculatory leukocyte activation and its association with glycocalyx degradation. In this prospective observational study, the microcirculation was assessed at the beginning of surgery (T0), end of surgery (T1) and 24 h after surgery (T2) using Incident Dark Field imaging. Changes in vessel density, blood flow and leukocyte behaviour were monitored, as well as clinical parameters. Syndecan-1 levels as a parameter of glycocalyx degradation were analysed. 19 patients were included. Sublingual microcirculation showed a significant increase in the number of rolling leukocytes between T0 and T1 (1.5 [0.7-1.8] vs. 3.7 [1.7-5.4] Ls/C-PCV/4 s respectively, p = 0.001), and remained high at T2 when compared to T0 (3.8 [3-8.5] Ls/C-PCV/4 s, p = 0.006). The microvascular flow decreased at T2 (2.4 ± 0.3 vs. baseline 2.8 ± 0.2, respectively, p < 0.01). Duration of vascular inflow occlusion was associated with significantly higher numbers of sublingual microcirculatory rolling leukocytes. Syndecan-1 increased from T0 to T1 (42 [25-56] vs. 107 [86-164] ng/mL, p < 0.001). The microcirculatory perfusion was characterized by low convection capacity and high number of rolling leukocytes. The ability to sublingually monitor the rolling behaviour of the microcirculatory leukocytes allows for early identification of patients at risk of increased inflammatory response following major liver resection.
Conflict of interest statement
Prof. Dr. Ince has developed SDF imaging and is listed as an inventor on related patents commercialized by MicroVision Medical (MVM) under a license from the Academic Medical Centre (AMC). Prof. Dr.Ince receives no royalties or any benefits from this license. He has been a consultant for MVM in the past, but has not been involved with this company for more than 7 years now and holds no shares or stock. Braedius Medical, a company owned by a relative of Prof. Dr. Ince, has developed and designed a third generation handheld microscope called CytoCam-IDF imaging. Prof. Dr. Ince has no financial relation with Braedius Medical of any sort, i.e., never owned shares, or received consultancy or speaker fees from Braedius Medical. Prof. Dr. Ince runs an internet site
Figures
References
-
- Man K, Liang T-B, Lo C-M, Liu C-L, Ng IO-LY, et al. Hepatic stress gene expression and ultrastructural features under intermittent Pringle manoeuvre. Hepatobil. Pancreat. Dis. Int. 2002;1(2):249–257. - PubMed
-
- Torzilli G, Procopio F, Donadon M, Del Fabbro D, Cimino M, et al. Safety of intermittent Pringle maneuver cumulative time exceeding 120 minutes in liver resection: A further step in favor of the “radical but conservative” policy. Ann. Surg. 2012;255(2):270–280. doi: 10.1097/SLA.0b013e318232b375. - DOI - PubMed
-
- Bagante F, Ruzzenente A, Beal EW, Campagnaro T, Merath K, et al. Complications after liver surgery: A benchmark analysis. HPB. 2019;10:20. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
