

Novel diagnostic and therapeutic techniques reveal changed metabolic profiles in recurrent focal segmental glomerulosclerosis
- PMID: 33633212
- PMCID: PMC7907124
- DOI: 10.1038/s41598-021-83883-w
Novel diagnostic and therapeutic techniques reveal changed metabolic profiles in recurrent focal segmental glomerulosclerosis
Erratum in
-
Author Correction: Novel diagnostic and therapeutic techniques reveal changed metabolic profiles in recurrent focal segmental glomerulosclerosis.Sci Rep. 2021 May 17;11(1):10693. doi: 10.1038/s41598-021-89610-9. Sci Rep. 2021. PMID: 34001993 Free PMC article. No abstract available.
Abstract
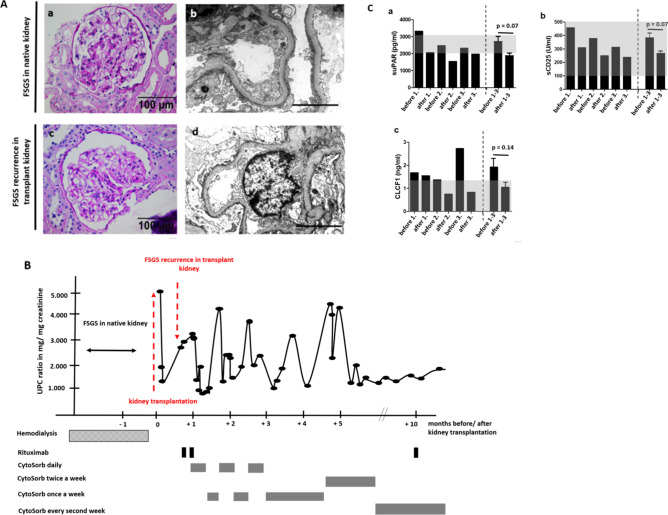
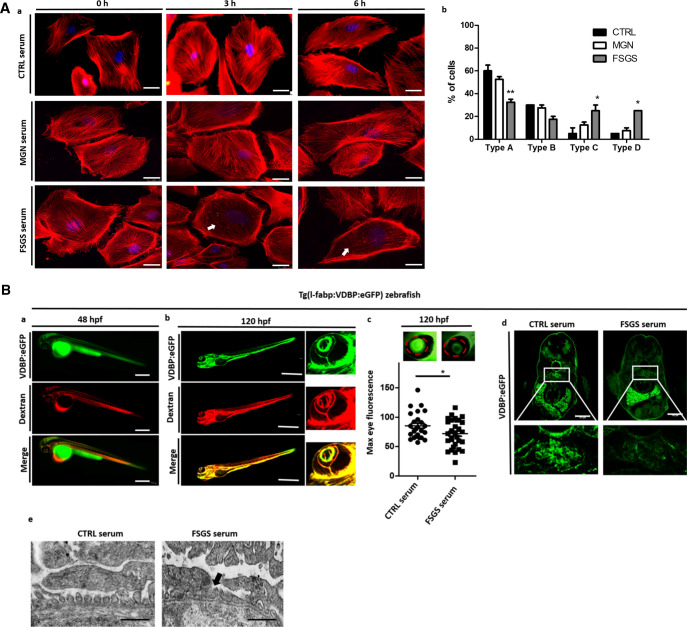
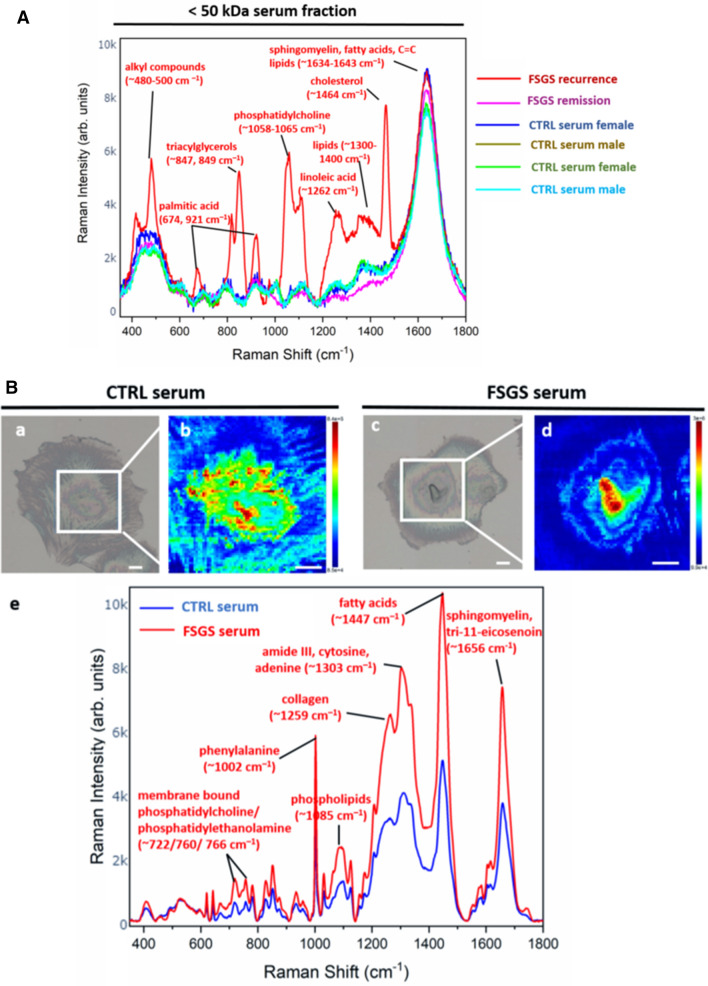
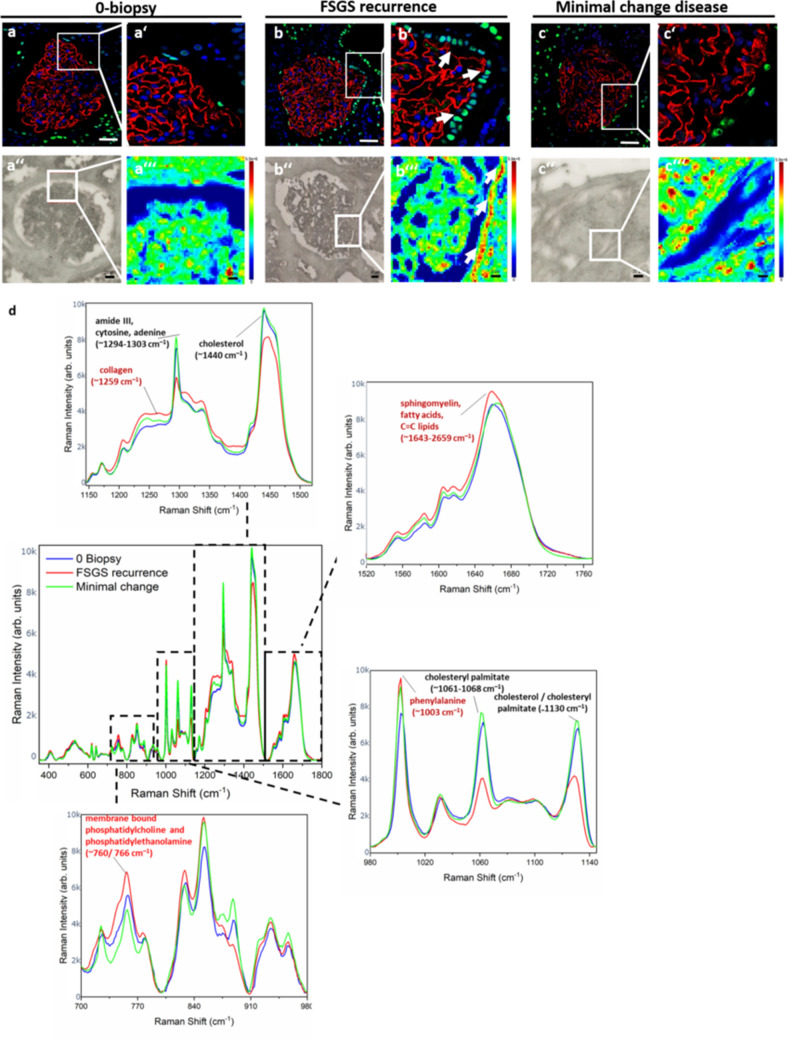
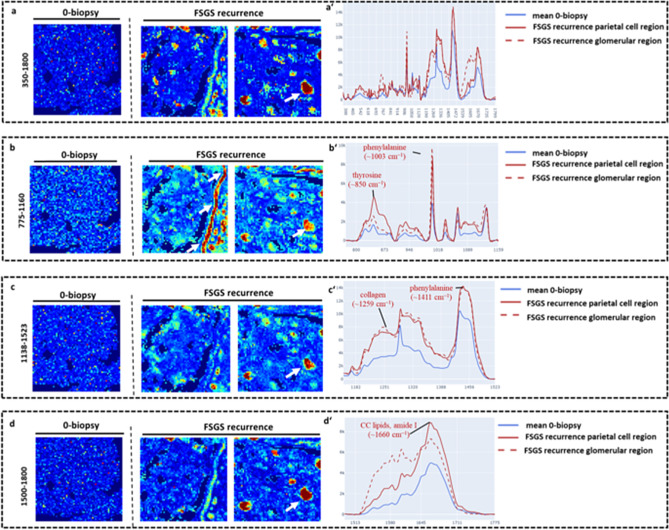
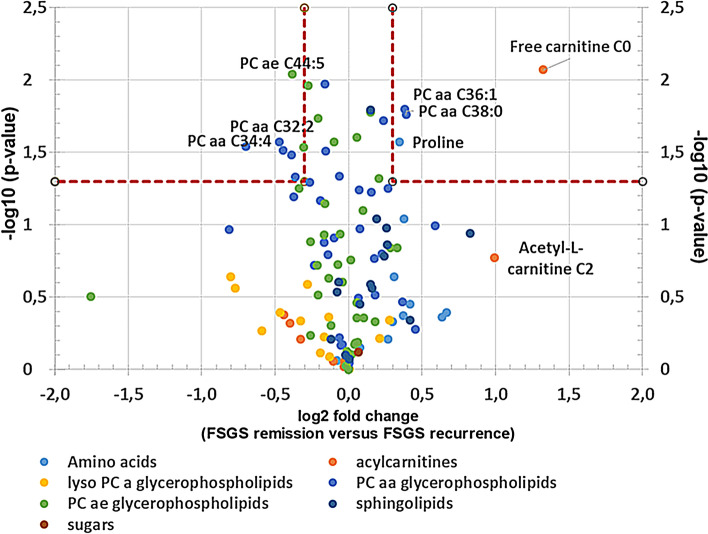
Idiopathic forms of Focal Segmental Glomerulosclerosis (FSGS) are caused by circulating permeability factors, which can lead to early recurrence of FSGS and kidney failure after kidney transplantation. In the past three decades, many research endeavors were undertaken to identify these unknown factors. Even though some potential candidates have been recently discussed in the literature, "the" actual factor remains elusive. Therefore, there is an increased demand in FSGS research for the use of novel technologies that allow us to study FSGS from a yet unexplored angle. Here, we report the successful treatment of recurrent FSGS in a patient after living-related kidney transplantation by removal of circulating factors with CytoSorb apheresis. Interestingly, the classical published circulating factors were all in normal range in this patient but early disease recurrence in the transplant kidney and immediate response to CytoSorb apheresis were still suggestive for pathogenic circulating factors. To proof the functional effects of the patient's serum on podocytes and the glomerular filtration barrier we used a podocyte cell culture model and a proteinuria model in zebrafish to detect pathogenic effects on the podocytes actin cytoskeleton inducing a functional phenotype and podocyte effacement. We then performed Raman spectroscopy in the < 50 kDa serum fraction, on cultured podocytes treated with the FSGS serum and in kidney biopsies of the same patient at the time of transplantation and at the time of disease recurrence. The analysis revealed changes in podocyte metabolome induced by the FSGS serum as well as in focal glomerular and parietal epithelial cell regions in the FSGS biopsy. Several altered Raman spectra were identified in the fractionated serum and metabolome analysis by mass spectrometry detected lipid profiles in the FSGS serum, which were supported by disturbances in the Raman spectra. Our novel innovative analysis reveals changed lipid metabolome profiles associated with idiopathic FSGS that might reflect a new subtype of the disease.
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
Podocyte foot process effacement in postreperfusion allograft biopsies correlates with early recurrence of proteinuria in focal segmental glomerulosclerosis.Transplantation. 2012 Jun 27;93(12):1238-44. doi: 10.1097/TP.0b013e318250234a. Transplantation. 2012. PMID: 22499148 Free PMC article.
-
Novel unbiased assay for circulating podocyte-toxic factors associated with recurrent focal segmental glomerulosclerosis.Am J Physiol Renal Physiol. 2016 May 15;310(10):F1148-56. doi: 10.1152/ajprenal.00349.2015. Epub 2015 Dec 30. Am J Physiol Renal Physiol. 2016. PMID: 26719363
-
Identification of glomerular and podocyte-specific genes and pathways activated by sera of patients with focal segmental glomerulosclerosis.PLoS One. 2019 Oct 3;14(10):e0222948. doi: 10.1371/journal.pone.0222948. eCollection 2019. PLoS One. 2019. PMID: 31581251 Free PMC article.
-
The role of podocyte injury in the pathogenesis of focal segmental glomerulosclerosis.Ren Fail. 2000 Nov;22(6):663-84. doi: 10.1081/jdi-100101955. Ren Fail. 2000. PMID: 11104157 Review.
-
Update on Recurrent Focal Segmental Glomerulosclerosis in Kidney Transplantation.Nephron. 2020;144 Suppl 1:65-70. doi: 10.1159/000510748. Epub 2020 Dec 1. Nephron. 2020. PMID: 33260184 Review.
Cited by
-
Novel mouse strains to study circulating permeability factor(s) in primary focal segmental glomerulosclerosis.PLoS One. 2022 Sep 22;17(9):e0274959. doi: 10.1371/journal.pone.0274959. eCollection 2022. PLoS One. 2022. PMID: 36137166 Free PMC article.
-
Potential biomarkers of recurrent FSGS: a review.BMC Nephrol. 2024 Aug 12;25(1):258. doi: 10.1186/s12882-024-03695-8. BMC Nephrol. 2024. PMID: 39134955 Free PMC article. Review.
-
Role of the Innate Immune Response in Glomerular Disease Pathogenesis: Focus on Podocytes.Cells. 2024 Jul 6;13(13):1157. doi: 10.3390/cells13131157. Cells. 2024. PMID: 38995008 Free PMC article. Review.
-
Kidney lipid dysmetabolism and lipid droplet accumulation in chronic kidney disease.Nat Rev Nephrol. 2023 Oct;19(10):629-645. doi: 10.1038/s41581-023-00741-w. Epub 2023 Jul 27. Nat Rev Nephrol. 2023. PMID: 37500941 Review.
-
Interaction of S100A6 Protein with the Four-Helical Cytokines.Biomolecules. 2023 Sep 4;13(9):1345. doi: 10.3390/biom13091345. Biomolecules. 2023. PMID: 37759746 Free PMC article.
References
-
- Kitiyakara C, Eggers P, Kopp JB. Twenty-one-year trend in ESRD due to focal segmental glomerulosclerosis in the United States. Am. J. Kidney Dis. 2004;44:815–825. - PubMed
-
- Haas M, Meehan SM, Karrison TG, Spargo BH. Changing etiologies of unexplained adult nephrotic syndrome: A comparison of renal biopsy findings from 1976–1979 and 1995–1997. Am. J. Kidney Dis. 1997;30:621–631. - PubMed
-
- Sethi S, Glassock RJ, Fervenza FC. Focal segmental glomerulosclerosis: Towards a better understanding for the practicing nephrologist. Nephrol. Dial. Transplant. 2015;30:375–384. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
Miscellaneous
