

Epidural Analgesia in Ventral Hernia Repair: An Analysis of 30-day Outcomes
- PMID: 33633416
- PMCID: PMC7901129
Epidural Analgesia in Ventral Hernia Repair: An Analysis of 30-day Outcomes
Abstract
Background: Ventral hernia repair (VHR) is a common procedure associated with significant postoperative morbidity and prolonged hospital length of stay (LOS). The use of epidural analgesia in VHR has not been widely evaluated.
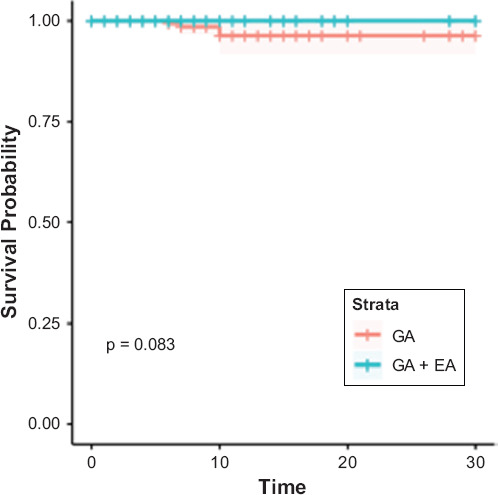
Purpose: To compare the outcomes of general anesthesia plus epidural analgesia (GA + EA) versus general anesthesia alone (GA) in patients undergoing ventral hernia repair.
Methods: The American College of Surgeons National Surgical Quality Improvement Program database was used to identify elective cases of VHR. Propensity score-matched analysis was used to compare outcomes in GA vs GA + EA groups. Cases receiving transverse abdominus plane blocks were excluded.
Results: A total of 9697 VHR cases were identified, resulting in two matched cohorts of 521 cases each. LOS was significantly longer in the GA + EA group (5.58 days) vs the GA group (5.20 days, p = 0.008). No other statistically significant differences in 30-day outcomes were observed between the matched cohorts.
Conclusion: Epidural analgesia in VHR is associated with statistically significant, but not clinically significant increase in LOS and may not yield any additional benefit in cases of isolated, elective VHR. Epidural analgesia may not be beneficial in this surgical population. Future studies should focus on alternative modes of analgesia to optimize pain control and outcomes for this procedure.
Keywords: anesthesia; complications; epidural; hernia; outcomes; regional; ventral.
Copyright © 1964–2019 by MedWorks Media Inc, Los Angeles, CA All rights reserved. Printed in the United States.
Figures
Similar articles
-
Is It Time to Reconsider Postoperative Epidural Analgesia in Patients Undergoing Elective Ventral Hernia Repair?: An AHSQC Analysis.Ann Surg. 2018 May;267(5):971-976. doi: 10.1097/SLA.0000000000002214. Ann Surg. 2018. PMID: 28288066
-
Comparative effectiveness of surgeon-performed transversus abdominis plane blocks and epidural catheters following open hernia repair with transversus abdominis release.Hernia. 2021 Dec;25(6):1611-1620. doi: 10.1007/s10029-021-02454-0. Epub 2021 Jul 28. Hernia. 2021. PMID: 34319465
-
Epidural analgesia and post-operative ileus after incisional hernia repair with transversus abdominis release: Results of a 5-year quality improvement initiative.Am J Surg. 2024 Apr;230:30-34. doi: 10.1016/j.amjsurg.2023.11.009. Epub 2023 Nov 11. Am J Surg. 2024. PMID: 38000938
-
Concomitant ventral hernia repair and bariatric surgery: a retrospective analysis from a UK-based bariatric center.Surg Endosc. 2019 Mar;33(3):705-710. doi: 10.1007/s00464-018-6492-6. Epub 2018 Oct 19. Surg Endosc. 2019. PMID: 30341658 Review.
-
Combined General/Epidural Anesthesia vs. General Anesthesia on Postoperative Cytokines: A Review and Meta-Analysis.Cancers (Basel). 2025 May 15;17(10):1667. doi: 10.3390/cancers17101667. Cancers (Basel). 2025. PMID: 40427164 Free PMC article. Review.
References
-
- Poulose BK, Shelton J, Phillips S, Moore D, Nealon W, Penson D, Beck W, Holzman MD. Epidemiology and cost of ventral hernia repair: making the case for hernia research. Hernia. 2012;16:179–183. - PubMed
-
- Faylona JM. Evolution of ventral hernia repair. Asian J Endosc Surg. 2017;10:252–258. - PubMed
-
- Bisgaard T, Kehlet H, Bay-Nielsen MB, Iversen MG, Wara P, Rosenberg J, Friis-Andersen HF, Jorgensen LN. Nationwide study of early outcomes after incisional hernia repair. Br J Surg. 2009;96:1452–1457. - PubMed
-
- Majumder A, Fayezizadeh M, Neupane R, Elliott HL, Novitsky YW. Benefits of multimodal enhanced recovery pathway in patients undergoing open ventral hernia repair. J Am Coll Surg. 2016;222:1106–1115. - PubMed
-
- Carli F, Mayo N, Klubien K, Schricker T, Trudel J, Belliveau P. Epidural analgesia enhances functional exercise capacity and health-related quality of life after colonic surgery: results of a randomized trial. Anesthesiology. 2002;97:540–549. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources