

Alternative flaps in autologous breast reconstruction
- PMID: 33634002
- PMCID: PMC7882326
- DOI: 10.21037/gs.2020.03.16
Alternative flaps in autologous breast reconstruction
Abstract
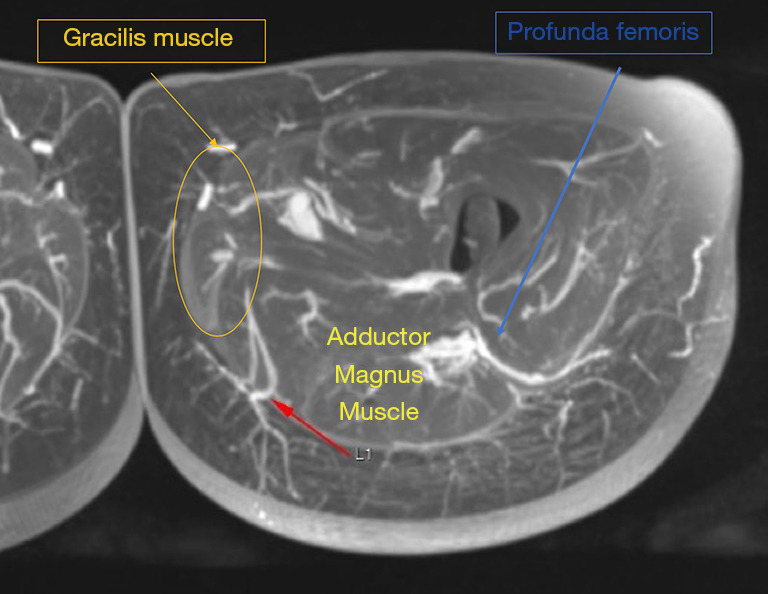
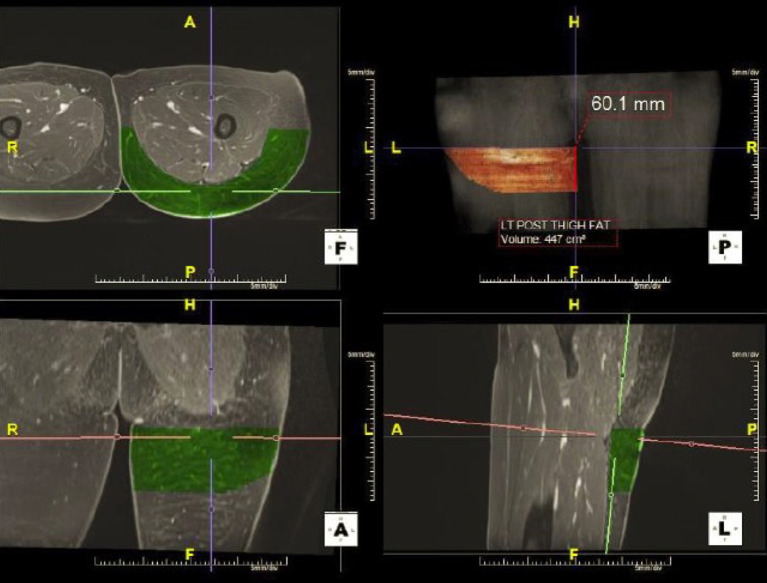
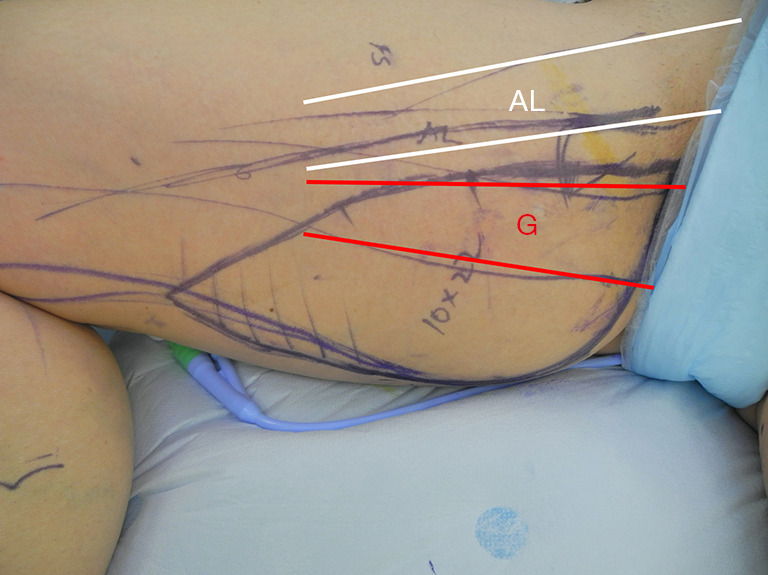
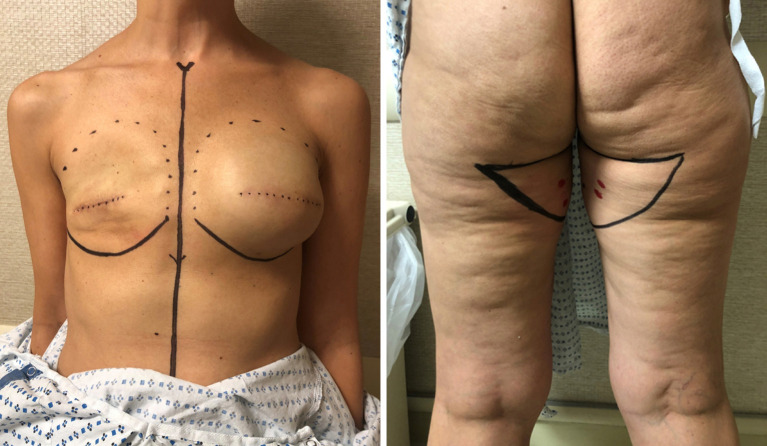
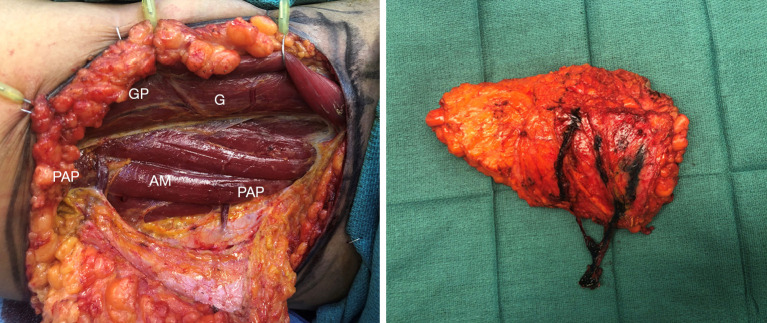
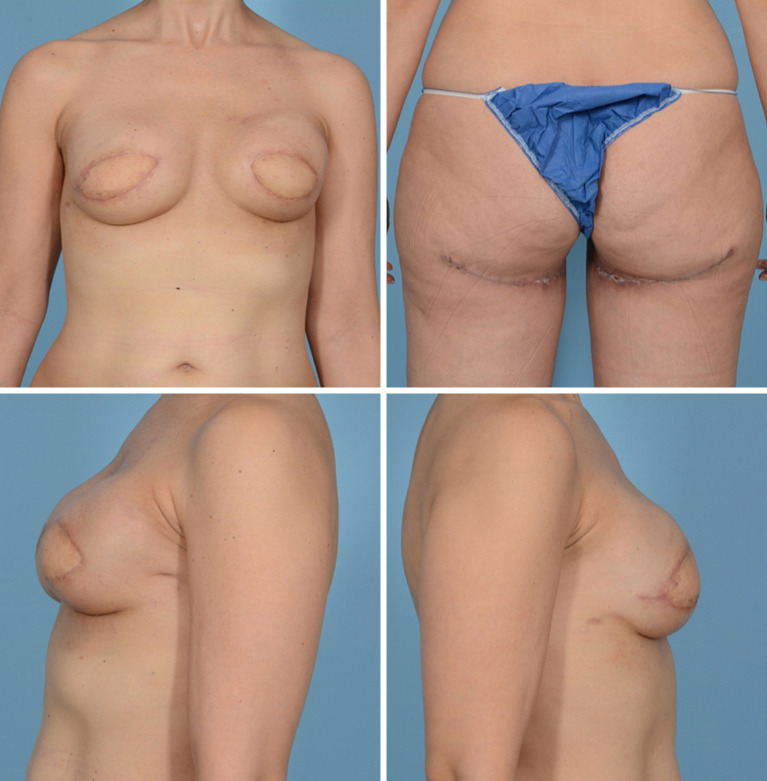
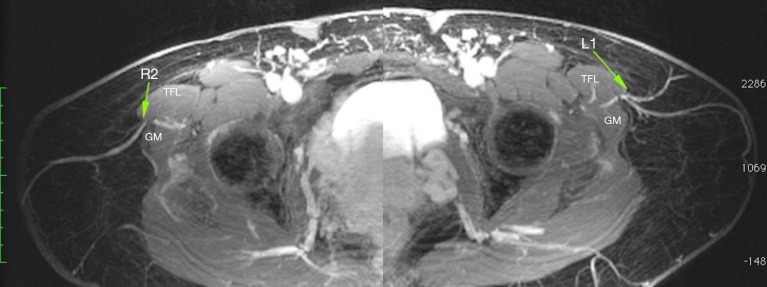
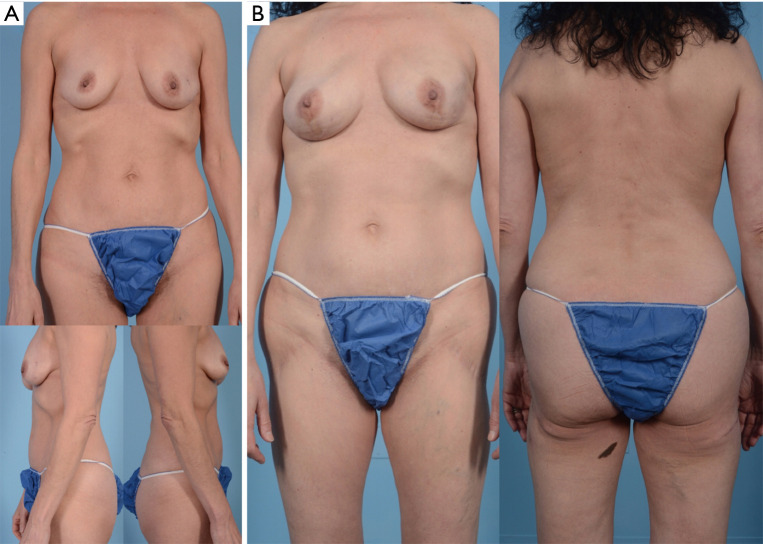
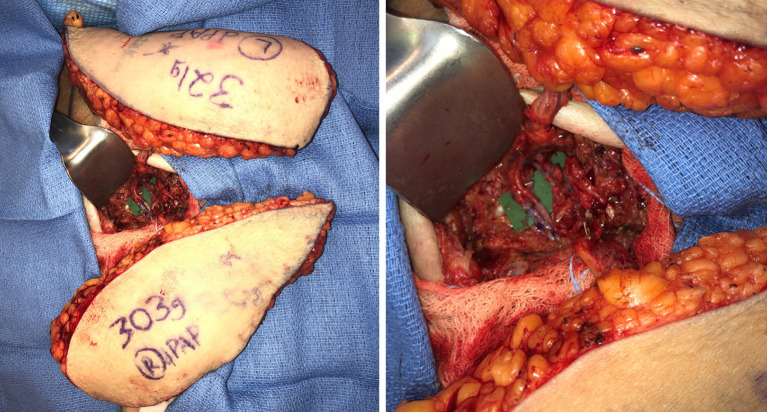
The gold standard for autologous reconstruction in the post-mastectomy patient remains the deep inferior epigastric artery perforator flap, although many women may not be candidates for abdominally based free tissue transfer. In this scenario, there are several other donor site options based from the thigh (transverse and diagonal upper gracilis flaps, profunda artery perforator flap, lateral thigh flap) and trunk (lumbar artery perforator flap, superior and inferior gluteal artery perforator flaps). This study will review the history, relevant anatomy, surgical technique and outcomes for alternative flaps in autologous reconstruction. Additionally, preoperative imaging (CTA, MRA) and novel applications (stacking flaps, neurotization) in breast reconstructive microsurgery will be discussed.
Keywords: Microsurgery; autologous tissue reconstruction; breast reconstruction.
2021 Gland Surgery. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at http://dx.doi.org/10.21037/gs.2020.03.16). The authors have no conflicts of interest to declare.
Figures




References
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources