

Histopathological Findings Predict Renal Recovery in Severe ANCA-Associated Vasculitis Requiring Intensive Care Treatment
- PMID: 33634143
- PMCID: PMC7900153
- DOI: 10.3389/fmed.2020.622028
Histopathological Findings Predict Renal Recovery in Severe ANCA-Associated Vasculitis Requiring Intensive Care Treatment
Abstract
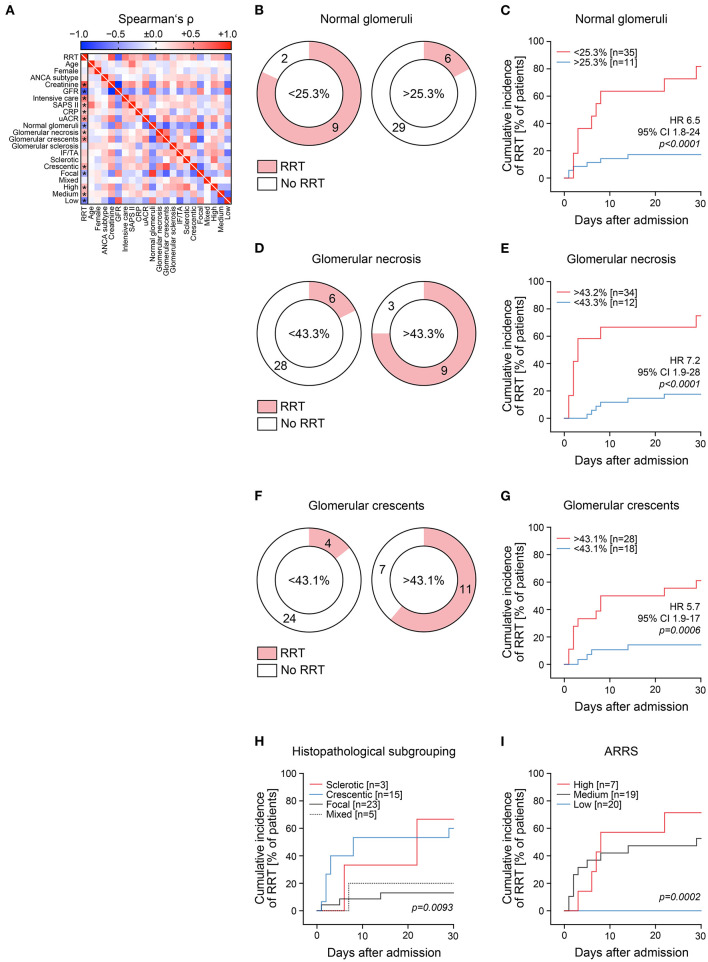
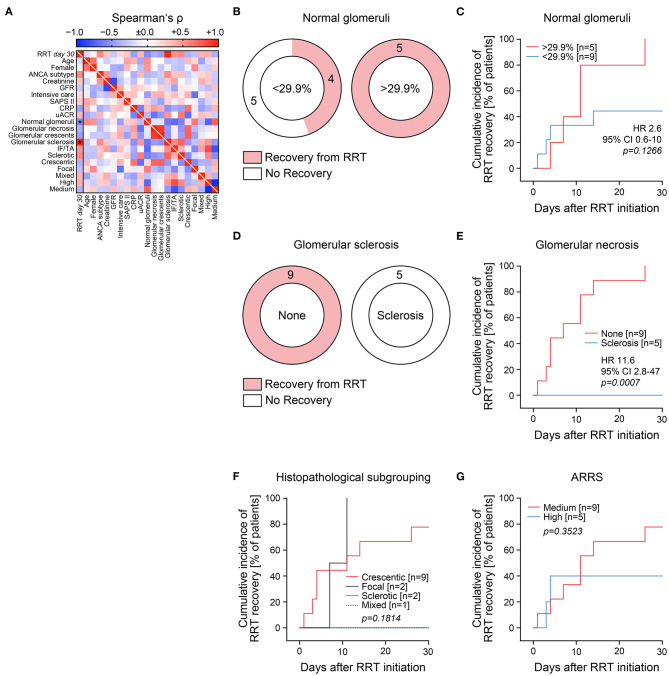
Renal involvement is a common and severe complication of AAV as it can cause ESRD. Histopathological subgrouping and ARRS are helpful to predict long-term ESRD in patients with AAV. Because a subgroup of critically ill patients with severe AAV present with deterioration of kidney function requiring RRT at admission, we here aimed to evaluate histopathological findings and predictive value of Berden's histopathological subgrouping and ARRS for severity of AKI and requirement of RRT during the short-term clinical course in critically ill patients requiring intensive care treatment and predictors for short-term renal recovery in patients requiring RRT. A subgroup of 15/46 (32. 6%) AAV patients with biopsy-proven AAV required RRT during the short-term course of disease, associated with requirement of critical care treatment. While histopathological subgrouping and ARRS were associated with requirement of acute RRT, presence of global glomerular scarring was the strongest predictor of failure to recover from RRT after initiation of remission induction therapy. This new aspect requires further investigation in a prospective controlled setting for therapeutic decision making especially in this subgroup.
Keywords: ANCA-associated vasculitis; acute kidney injury; autoimmune diseases; inflammation; intensive care treatment; renal replacement therapy; systemic vasculitis.
Copyright © 2021 Hakroush, Tampe, Korsten, Ströbel, Zeisberg and Tampe.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Consideration of Therapeutic Plasma Exchange in Association With Inflammatory Lesions in ANCA-Associated Glomerulonephritis: A Real-World Retrospective Study From a Single Center.Front Immunol. 2021 Jun 17;12:645483. doi: 10.3389/fimmu.2021.645483. eCollection 2021. Front Immunol. 2021. PMID: 34220805 Free PMC article.
-
Characteristics and Outcomes of Granulomatosis With Polyangiitis (Wegener) and Microscopic Polyangiitis Requiring Renal Replacement Therapy: Results From the European Renal Association-European Dialysis and Transplant Association Registry.Am J Kidney Dis. 2015 Oct;66(4):613-20. doi: 10.1053/j.ajkd.2015.03.025. Epub 2015 May 12. Am J Kidney Dis. 2015. PMID: 25975963
-
Clinical presentation and outcome prediction of clinical, serological, and histopathological classification schemes in ANCA-associated vasculitis with renal involvement.Clin Rheumatol. 2016 Jul;35(7):1805-16. doi: 10.1007/s10067-016-3195-z. Epub 2016 Feb 6. Clin Rheumatol. 2016. PMID: 26852317
-
ANCA-associated vasculitis with renal involvement.J Nephrol. 2018 Apr;31(2):197-208. doi: 10.1007/s40620-017-0412-z. Epub 2017 May 30. J Nephrol. 2018. PMID: 28560688 Review.
-
Effects of renal replacement therapy on renal recovery after acute kidney injury.Nephron Clin Pract. 2014;127(1-4):35-41. doi: 10.1159/000363671. Epub 2014 Sep 24. Nephron Clin Pract. 2014. PMID: 25343818 Review.
Cited by
-
Proteinuria Indicates Decreased Normal Glomeruli in ANCA-Associated Glomerulonephritis Independent of Systemic Disease Activity.J Clin Med. 2021 Apr 6;10(7):1538. doi: 10.3390/jcm10071538. J Clin Med. 2021. PMID: 33917561 Free PMC article.
-
Low levels of hemoglobin associate with critical illness and predict disease course in patients with ANCA-associated renal vasculitis.Sci Rep. 2022 Nov 4;12(1):18736. doi: 10.1038/s41598-022-23313-7. Sci Rep. 2022. PMID: 36333432 Free PMC article.
-
Systematic Histological Scoring Reveals More Prominent Interstitial Inflammation in Myeloperoxidase-ANCA Compared to Proteinase 3-ANCA Glomerulonephritis.J Clin Med. 2021 Mar 16;10(6):1231. doi: 10.3390/jcm10061231. J Clin Med. 2021. PMID: 33809645 Free PMC article.
-
Comprehensive Analysis of Sex Differences at Disease Manifestation in ANCA-Associated Glomerulonephritis.Front Immunol. 2021 Sep 23;12:736638. doi: 10.3389/fimmu.2021.736638. eCollection 2021. Front Immunol. 2021. PMID: 34630417 Free PMC article.
-
Low hemoglobin levels are associated with Bowman's capsule rupture and peritubular capillaritis in ANCA-associated renal vasculitis: a link of vascular injury to anemia?J Nephrol. 2023 Nov;36(8):2305-2316. doi: 10.1007/s40620-023-01748-z. Epub 2023 Sep 7. J Nephrol. 2023. PMID: 37676636 Free PMC article.
References
-
- Pettersson EE, Sundelin B, Heigl Z. Incidence and outcome of pauci-immune necrotizing and crescentic glomerulonephritis in adults. Clin Nephrol. (1995) 43:141–9. - PubMed
-
- Hruskova Z, Stel VS, Jayne D, Aasarod K, De Meester J, Ekstrand A, et al. . Characteristics and outcomes of granulomatosis with polyangiitis (Wegener) and microscopic polyangiitis requiring renal replacement therapy: results from the European renal association-European dialysis and transplant association registry. Am J Kidney Dis. (2015) 66:613–20. 10.1053/j.ajkd.2015.03.025 - DOI - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources