

Cinematic Rendering in Mixed-Reality Holograms: A New 3D Preoperative Planning Tool in Pediatric Heart Surgery
- PMID: 33634174
- PMCID: PMC7900175
- DOI: 10.3389/fcvm.2021.633611
Cinematic Rendering in Mixed-Reality Holograms: A New 3D Preoperative Planning Tool in Pediatric Heart Surgery
Abstract
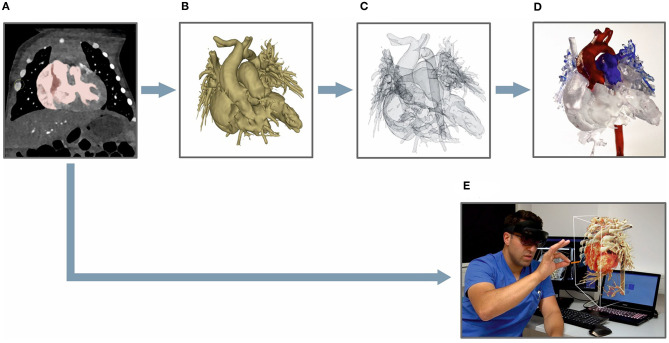
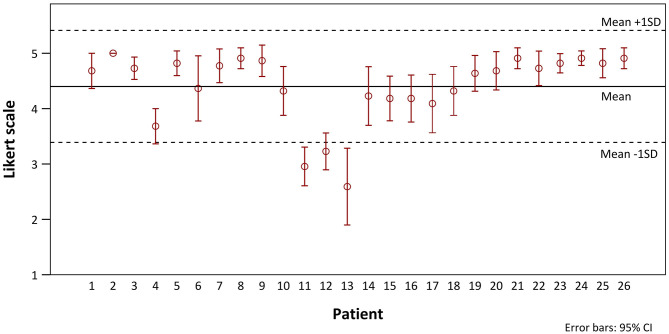
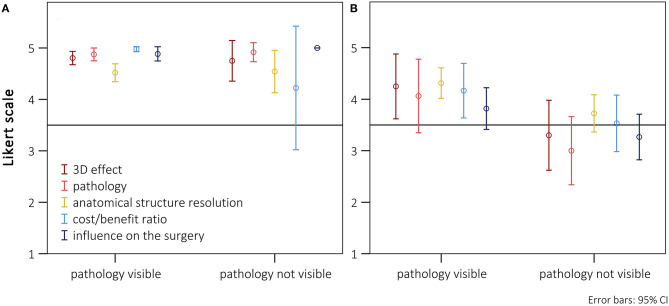
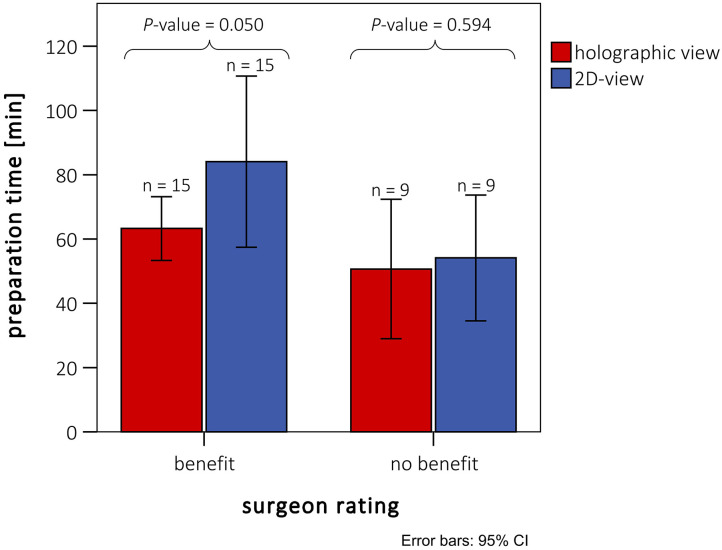
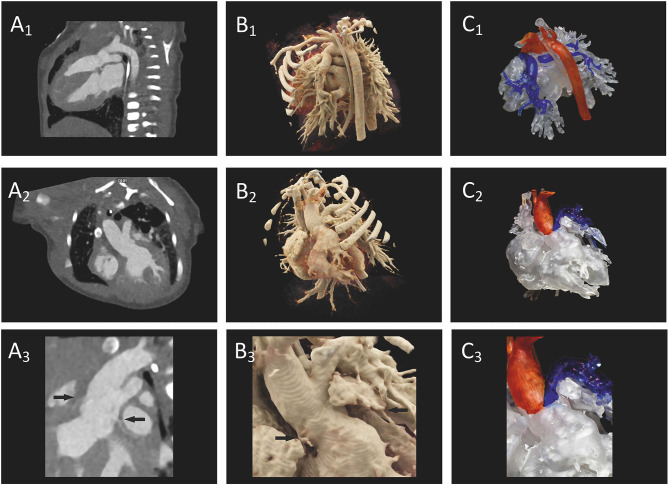
Cinematic rendering (CR) is based on a new algorithm that creates a photo-realistic three-dimensional (3D) picture from cross-sectional images. Previous studies have shown its positive impact on preoperative planning. To date, CR presentation has only been possible on 2D screens which limited natural 3D perception. To depict CR-hearts spatially, we used mixed-reality technology and mapped corresponding hearts as holograms in 3D space. Our aim was to assess the benefits of CR-holograms in the preoperative planning of cardiac surgery. Including 3D prints allowed a direct comparison of two spatially resolved display methods. Twenty-six patients were recruited between February and September 2019. CT or MRI was used to visualize the patient's heart preoperatively. The surgeon was shown the anatomy in cross-sections on a 2D screen, followed by spatial representations as a 3D print and as a high-resolution hologram. The holographic representation was carried out using mixed-reality glasses (HoloLens®). To create the 3D prints, corresponding structures were segmented to create STL files which were printed out of resin. In 22 questions, divided in 5 categories (3D-imaging effect, representation of pathology, structure resolution, cost/benefit ratio, influence on surgery), the surgeons compared each spatial representation with the 2D method, using a five-level Likert scale. The surgical preparation time was assessed by comparing retrospectively matched patient pairs, using a paired t-test. CR-holograms surpassed 2D-monitor imaging in all categories. CR-holograms were superior to 3D prints in all categories (mean Likert scale 4.4 ± 1.0 vs. 3.7 ± 1.3, P < 0.05). Compared to 3D prints it especially improved the depth perception (4.7 ± 0.7 vs. 3.7 ± 1.2) and the representation of the pathology (4.4 ± 0.9 vs. 3.6 ± 1.2). 3D imaging reduced the intraoperative preparation time (n = 24, 59 ± 23 min vs. 73 ± 43 min, P < 0.05). In conclusion, the combination of an extremely photo-realistic presentation via cinematic rendering and the spatial presentation in 3D space via mixed-reality technology allows a previously unattained level of comprehension of anatomy and pathology in preoperative planning.
Keywords: 3D printing; cinematic rendering; congenital heart disease; mixed-reality; pediatric heart surgery; preoperative planning.
Copyright © 2021 Gehrsitz, Rompel, Schöber, Cesnjevar, Purbojo, Uder, Dittrich and Alkassar.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures

References
LinkOut - more resources
Full Text Sources
Other Literature Sources