

An unusual case of apical myocarditis: a case report
- PMID: 33634222
- PMCID: PMC7891283
- DOI: 10.1093/ehjcr/ytaa347
An unusual case of apical myocarditis: a case report
Abstract
Background: Myocardial infarction with non-obstructed coronary arteries (MINOCA) syndrome accounts for ∼6-8% of acute coronary syndrome presentations. Historically, MINOCA has been thought of as a benign condition, however, recent evidence suggests that some aetiologies of MINOCA such as cardiomyopathies are associated with significantly higher mortality than other causes such as myocarditis. Therefore, identifying the underlying cause of MINOCA is important in determining patient management and prognosis.
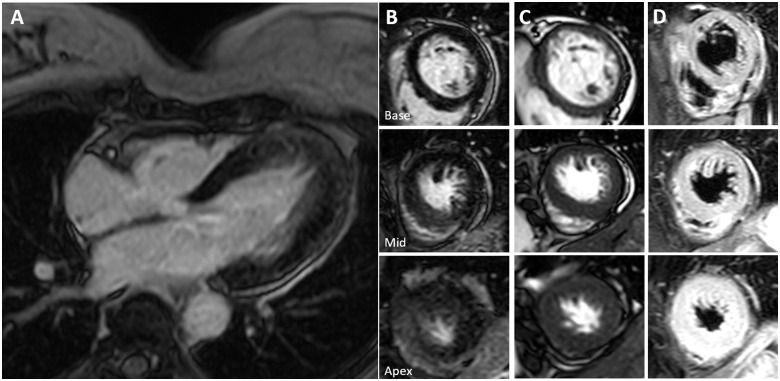
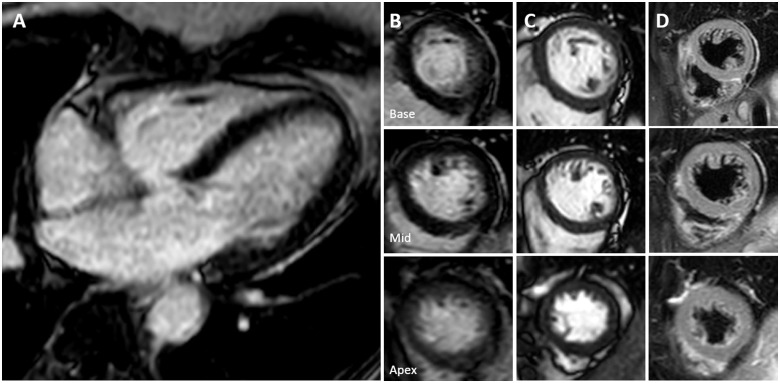
Case summary: We describe the case of a 58-year-old lady with an acute admission with MINOCA syndrome. Cardiac magnetic resonance (CMR) examination on Day 9 demonstrated hypertrophy of the apical segments of the left ventricle (LV), with diffuse mid-wall hyper-enhancement on late gadolinium enhancement (LGE) images. T2-weighted imaging was suggestive of active inflammation in the hypertrophied segments. A repeat CMR scan was performed 3 months later showed normalization of LV wall thickness, LGE and T2 values in the apical segments.
Discussion: This case report highlights the benefits of CMR with oedema-weighted imaging in the acute stages of MINOCA syndrome, as well as the importance of serial imaging in this patient cohort. While baseline imaging raised the possibility of apical hypertrophic cardiomyopathy, resolution of apical hypertrophy on follow-up CMR showed that the patient had acute myocarditis, specifically involving the apical segments.
Keywords: Cardiac magnetic resonance; Case report; MINOCA syndrome; Myocarditis; T2-weighted imaging; Takotsubo.
© The Author(s) 2020. Published by Oxford University Press on behalf of the European Society of Cardiology.
Figures

Similar articles
-
Characterisation of patients with and without cardiac magnetic resonance imaging abnormalities presenting with myocardial infarction with non-obstructive coronary arteries (MINOCA).Acta Cardiol. 2021 Sep;76(7):760-768. doi: 10.1080/00015385.2020.1785134. Epub 2020 Jun 29. Acta Cardiol. 2021. PMID: 32594904
-
Prognostic Value of Cardiac Magnetic Resonance Imaging in Patients With a Working Diagnosis of MINOCA-An Outcome Study With up to 10 Years of Follow-Up.Circ Cardiovasc Imaging. 2023 Aug;16(8):e014454. doi: 10.1161/CIRCIMAGING.122.014454. Epub 2023 Aug 15. Circ Cardiovasc Imaging. 2023. PMID: 37582156
-
Coronary Optical Coherence Tomography and Cardiac Magnetic Resonance Imaging to Determine Underlying Causes of Myocardial Infarction With Nonobstructive Coronary Arteries in Women.Circulation. 2021 Feb 16;143(7):624-640. doi: 10.1161/CIRCULATIONAHA.120.052008. Epub 2020 Nov 14. Circulation. 2021. PMID: 33191769 Free PMC article.
-
Medium-Term Prognostic Implications of Cardiac Magnetic Resonance Imaging in Patients With Myocardial Infarction With Nonobstructive Coronary Arteries (MINOCA): A Systematic Review and Meta-Analysis.Heart Lung Circ. 2023 Nov;32(11):1334-1346. doi: 10.1016/j.hlc.2023.09.007. Epub 2023 Oct 31. Heart Lung Circ. 2023. PMID: 37919116
-
Diagnostic and Prognostic Role of Cardiac Magnetic Resonance in MINOCA: Systematic Review and Meta-Analysis.JACC Cardiovasc Imaging. 2023 Mar;16(3):376-389. doi: 10.1016/j.jcmg.2022.12.029. JACC Cardiovasc Imaging. 2023. PMID: 36889851
References
-
- Scalone G, Niccoli G, Crea F.. Editor’s choice—pathophysiology, diagnosis and management of MINOCA: an update. Eur Heart J Acute Cardiovasc Care 2019;8:54–62. - PubMed
-
- Agewall S, Beltrame JF, Reynolds HR, Niessner A, Rosano G, Caforio ALP. et al. ESC working group position paper on myocardial infarction with non-obstructive coronary arteries. Eur Heart J 2017;38:143–153. - PubMed
-
- Ferreira VM, Schulz-Menger J, Holmvang G, Kramer CM, Carbone I, Sechtem U. et al. Cardiovascular magnetic resonance in nonischemic myocardial inflammation: expert recommendations. J Am Coll Cardiol 2018;72:3158–3176. - PubMed
-
- Thygesen K, Alpert JS, Jaffe AS, Chaitman BR, Bax JJ, Morrow DA. et al. Fourth universal definition of myocardial infarction (2018). Russ J Cardiol 2019;40:237–269. - PubMed
-
- Pasupathy S, Air T, Dreyer RP, Tavella R, Beltrame JF.. Systematic review of patients presenting with suspected myocardial infarction and nonobstructive coronary arteries. Circulation 2015;131:861–870. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources