

Effects of Volatile Anesthetics on Postoperative Ischemic Stroke Incidence
- PMID: 33634705
- PMCID: PMC8174248
- DOI: 10.1161/JAHA.120.018952
Effects of Volatile Anesthetics on Postoperative Ischemic Stroke Incidence
Abstract
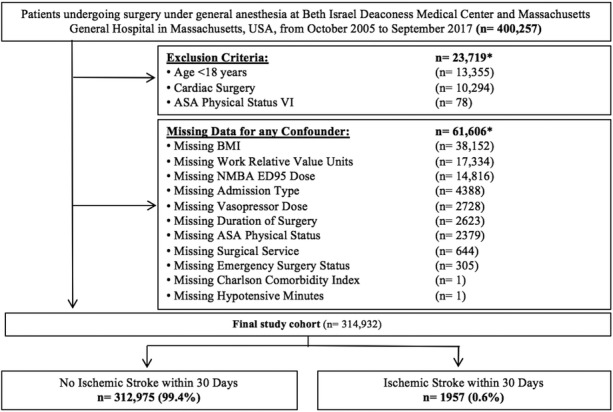
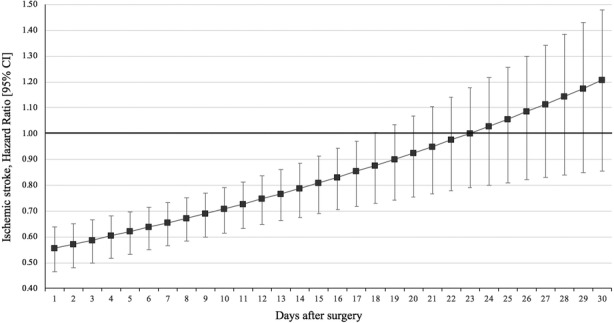
Background Preclinical studies suggest that volatile anesthetics decrease infarct volume and improve the outcome of ischemic stroke. This study aims to determine their effect during noncardiac surgery on postoperative ischemic stroke incidence. Methods and Results This was a retrospective cohort study of surgical patients undergoing general anesthesia at 2 tertiary care centers in Boston, MA, between October 2005 and September 2017. Exclusion criteria comprised brain death, age <18 years, cardiac surgery, and missing covariate data. The exposure was defined as median age-adjusted minimum alveolar concentration of all intraoperative measurements of desflurane, sevoflurane, and isoflurane. The primary outcome was postoperative ischemic stroke within 30 days. Among 314 932 patients, 1957 (0.6%) experienced the primary outcome. Higher doses of volatile anesthetics had a protective effect on postoperative ischemic stroke incidence (adjusted odds ratio per 1 minimum alveolar concentration increase 0.49, 95% CI, 0.40-0.59, P<0.001). In Cox proportional hazards regression, the effect was observed for 17 postoperative days (postoperative day 1: hazard ratio (HR), 0.56; 95% CI, 0.48-0.65; versus day 17: HR, 0.85; 95% CI, 0.74-0.99). Volatile anesthetics were also associated with lower stroke severity: Every 1-unit increase in minimum alveolar concentration was associated with a 0.006-unit decrease in the National Institutes of Health Stroke Scale (95% CI, -0.01 to -0.002, P=0.002). The effects were robust throughout various sensitivity analyses including adjustment for anesthesia providers as random effect. Conclusions Among patients undergoing noncardiac surgery, volatile anesthetics showed a dose-dependent protective effect on the incidence and severity of early postoperative ischemic stroke.
Keywords: anesthetics; cerebral ischemia; retrospective studies; stroke; stroke prevention.
Conflict of interest statement
Dr Hanafy reports a grant by the NIH (grant no. R01NS109174). Dr Houle reports grants from the National Institute of Neurological Disorders and Stroke (NINDS; PI), grants from the National Institute of General Medical Sciences (NIGMS), personal fees from Headache, personal fees from Anesthesiology, and personal fees from Cephalalgia, outside the submitted work. Dr Eikermann received funding for investigator‐initiated trials from Merck and honorarium for giving advice to Merck, and a grant by the NIH (grant no. UG3HL140177); he is an Associate Editor of the
Figures
References
-
- Preventing, and managing the impact of, anesthesia awareness. Sentinel Event Alert. 2004;32: 1–3. - PubMed
-
- Selim M. Perioperative stroke. N Engl J Med. 2007;356:706–713. - PubMed
-
- Mashour GA, Moore LE, Lele AV, Robicsek SA, Gelb AW. Perioperative care of patients at high risk for stroke during or after non‐cardiac, non‐neurologic surgery: consensus statement from the Society for Neuroscience in Anesthesiology and Critical Care. J Neurosurg Anesthesiol. 2014;26:273–285. - PubMed
-
- Zausinger S, Baethmann A, Schmid‐Elsaesser R. Anesthetic methods in rats determine outcome after experimental focal cerebral ischemia: mechanical ventilation is required to obtain controlled experimental conditions. Brain Res Brain Res Protoc. 2002;9:112–121. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
