

Evaluation of Exercise Interventions and Outcomes After Hip Arthroplasty: A Systematic Review and Meta-analysis
- PMID: 33635329
- PMCID: PMC7910817
- DOI: 10.1001/jamanetworkopen.2021.0254
Evaluation of Exercise Interventions and Outcomes After Hip Arthroplasty: A Systematic Review and Meta-analysis
Abstract
Importance: Preoperative and postoperative exercise interventions are commonly used in patients with total hip arthroplasty despite a lack of established efficacy.
Objective: To explore clinical outcomes associated with exercise training before and after hip arthroplasty.
Data sources: PubMed, Cochrane Central Register of Controlled Trials, Cumulative Index to Nursing and Allied Health Literature, EMBASE, and Google Scholar were searched from their inception to March 2020. Reference lists of included trials and related reviews were also searched.
Study selection: Randomized clinical trials of land-based exercise interventions before or after total hip arthroplasty were included.
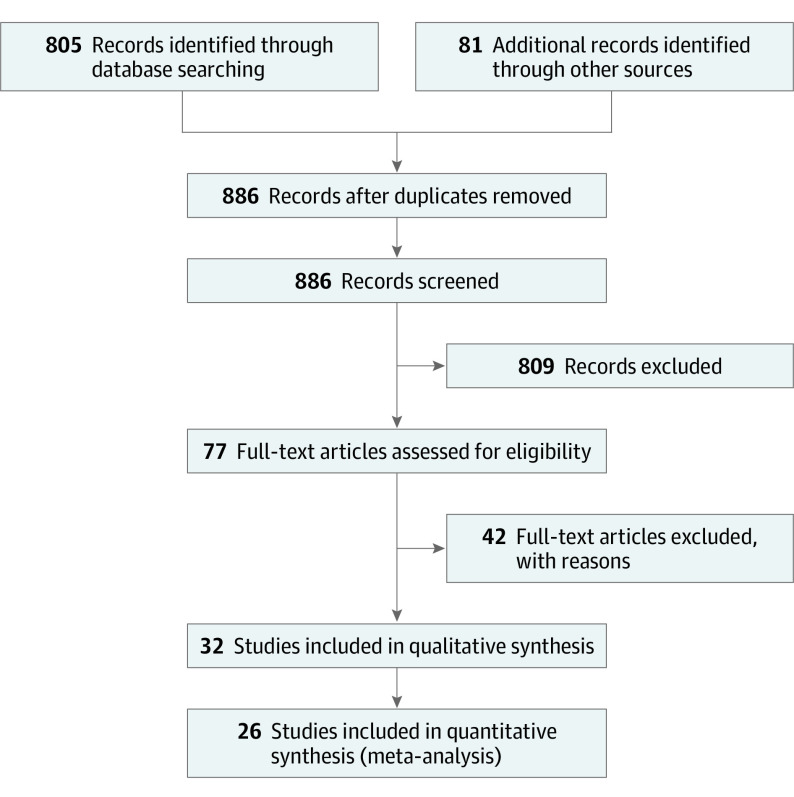
Data extraction and synthesis: This systematic review and meta-analysis is reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) reporting guideline. Data extraction was independently performed in duplicate. Random-effects meta-analyses with restricted maximum likelihood were performed for pooling the data.
Main outcomes and measures: The primary prespecified outcome was self-reported physical function. Secondary prespecified outcomes were self-reported pain intensity, quality of life, gait speed, lower body muscle strength, lower body flexibility, anxiety, hospital length of stay, and adverse events.
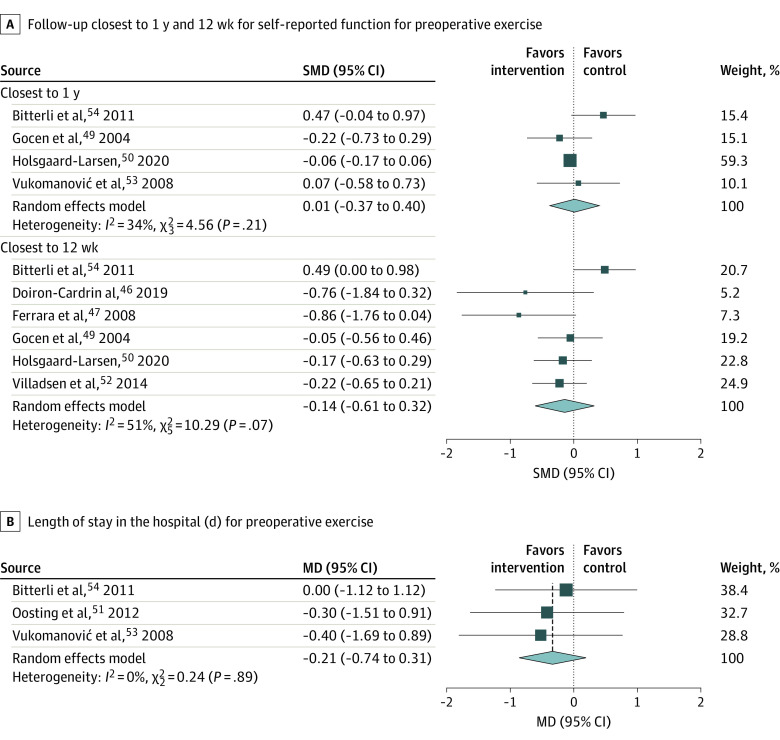
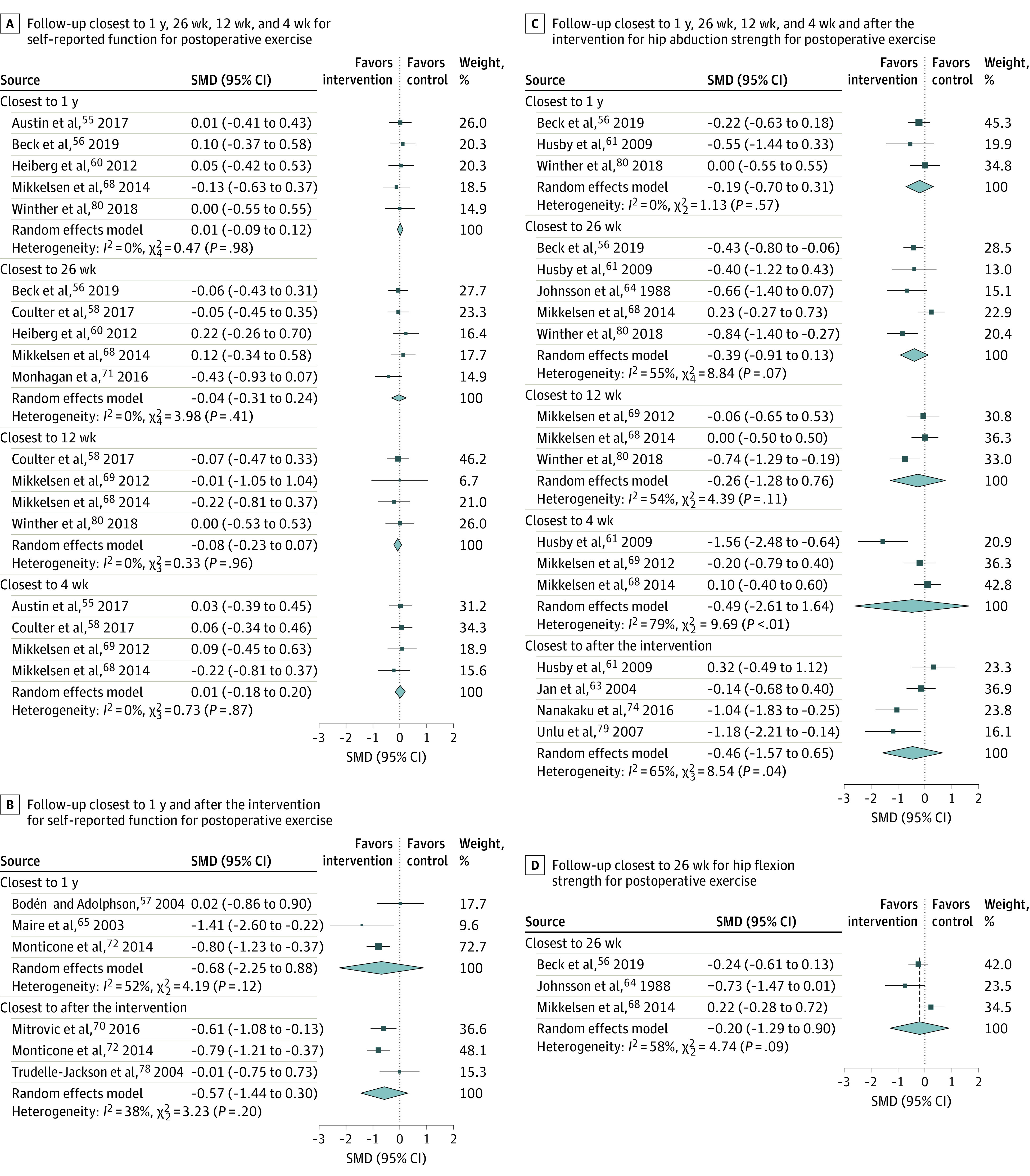
Results: A total of 32 randomized clinical trials with 1753 patients were included in the qualitative synthesis, and 26 studies with 1004 patients were included in the meta-analysis. Compared with usual care or no or minimal intervention, postoperative exercise training was not associated with improved self-reported physical function, with a moderate level of certainty, at 4 weeks (standardized mean difference [SMD], 0.01; 95% CI, -0.18 to 0.20), 12 weeks (SMD, -0.08; 95% CI, -0.23 to 0.07) and 26 weeks (SMD, -0.04; 95% CI, -0.31 to 0.24) postoperatively, and low level of certainty at 1 year after surgical treatment (SMD, 0.01; 95% CI, -0.09 to 0.12). For preoperative exercise interventions, there was no association of exercised training with self-reported physical function compared with the control at the 12-week (SMD, -0.14; 95% CI, -0.61 to 0.32) or 1-year follow-ups (SMD, 0.01; 95% CI, -0.37 to 0.40) with very low certainty, and no association with length of stay (mean difference, -0.21; 95% CI, -0.74 to 0.31) at moderate certainty. Results for postoperative hip muscle strength were rated at very low certainty, with no statistical significance. Meta-analysis could not be performed for other outcomes.
Conclusions and relevance: This systematic review and meta-analysis found low- to moderate-quality evidence that postoperative exercise interventions were not associated with improved self-reported physical function compared with usual care or no or minimal intervention. Furthermore, there was very low-quality evidence that preoperative exercise programs were not associated with higher self-reported physical function and hospital length of stay compared with usual care or no or minimal intervention.
Conflict of interest statement
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
