

Central venous pressure swing outperforms diaphragm ultrasound as a measure of inspiratory effort during pressure support ventilation in COVID-19 patients
- PMID: 33635495
- PMCID: PMC7908005
- DOI: 10.1007/s10877-021-00674-4
Central venous pressure swing outperforms diaphragm ultrasound as a measure of inspiratory effort during pressure support ventilation in COVID-19 patients
Abstract
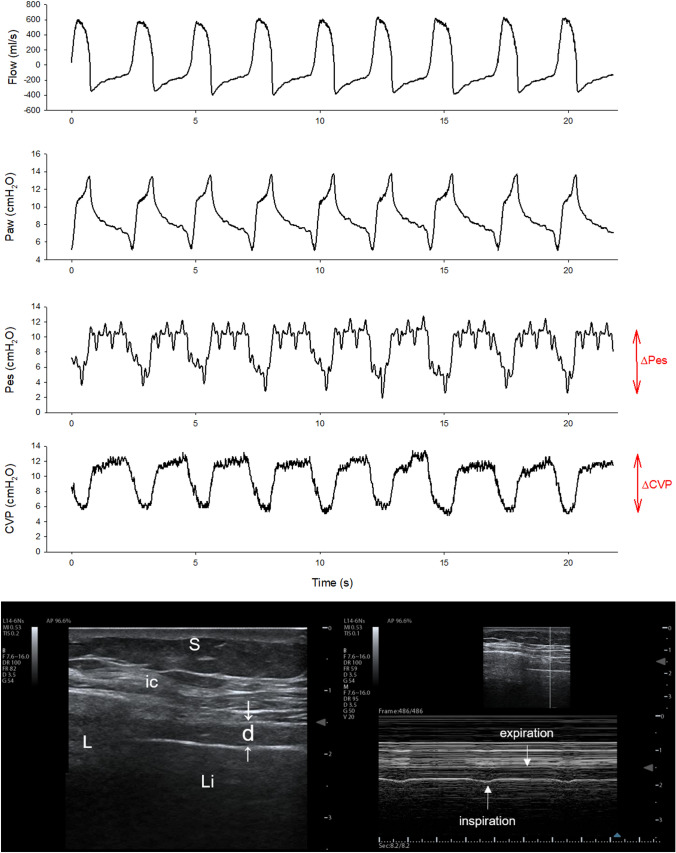
Purpose: The COVID-19-related shortage of ICU beds magnified the need of tools to properly titrate the ventilator assistance. We investigated whether bedside-available indices such as the ultrasonographic changes in diaphragm thickening ratio (TR) and the tidal swing in central venous pressure (ΔCVP) are reliable estimates of inspiratory effort, assessed as the tidal swing in esophageal pressure (ΔPes).
Methods: Prospective, observational clinical investigation in the intensive care unit of a tertiary care Hospital. Fourteen critically-ill patients were enrolled (age 64 ± 7 years, BMI 29 ± 4 kg/m2), after 6 [3; 9] days from onset of assisted ventilation. A three-level pressure support trial was performed, at 10 (PS10), 5 (PS5) and 0 cmH2O (PS0). In each step, the esophageal and central venous pressure tidal swing were recorded, as well as diaphragm ultrasound.
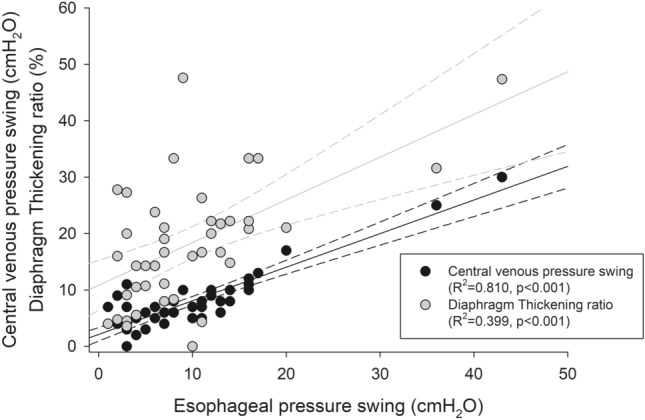
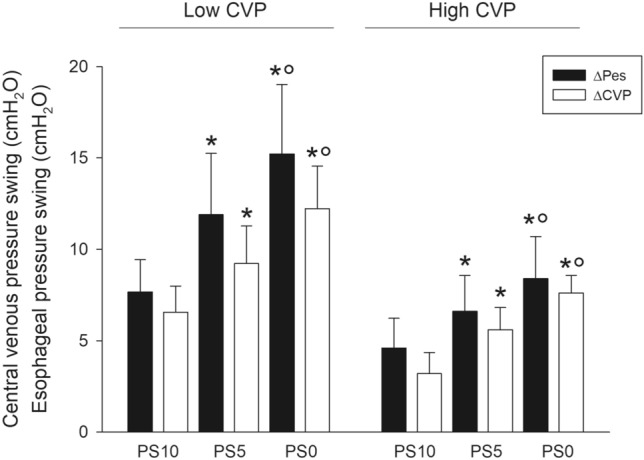
Results: The reduction of pressure support was associated with an increased respiratory rate and a reduced tidal volume, while minute ventilation was unchanged. ΔPes significantly increased with reducing support (5 [3; 8] vs. 8 [14; 13] vs. 12 [6; 16] cmH2O, p < 0.0001), as did the diaphragm TR (9.2 ± 6.1 vs. 17.6 ± 7.2 vs. 28.0 ± 10.0%, p < 0.0001) and the ΔCVP (4 [3; 7] vs. 8 [5; 9] vs. 10 [7; 11] cmH2O, p < 0.0001). ΔCVP was significantly associated with ΔPes (R2 = 0.810, p < 0.001), as was diaphragm TR, albeit with a lower coefficient of determination (R2 = 0.399, p < 0.001).
Conclusions: In patients with COVID-19-associated respiratory failure undergoing assisted mechanical ventilation, ΔCVP is a better estimate of inspiratory effort than diaphragm ultrasound.
Keywords: COVID-19; Diaphragm ultrasound; Esophageal pressure; Pressure support ventilation; Weaning.
© 2021. The Author(s).
Conflict of interest statement
The authors have no conflicts of interest to declare that are relevant to the content of this article/
Figures

Similar articles
-
Assessment of Inspiratory Effort in Spontaneously Breathing COVID-19 ARDS Patients Undergoing Helmet CPAP: A Comparison between Esophageal, Transdiaphragmatic and Central Venous Pressure Swing.Diagnostics (Basel). 2023 Jun 5;13(11):1965. doi: 10.3390/diagnostics13111965. Diagnostics (Basel). 2023. PMID: 37296817 Free PMC article.
-
Oesophageal pressure and respiratory muscle ultrasonographic measurements indicate inspiratory effort during pressure support ventilation.Br J Anaesth. 2020 Jul;125(1):e148-e157. doi: 10.1016/j.bja.2020.02.026. Epub 2020 May 6. Br J Anaesth. 2020. PMID: 32386831
-
Diaphragm ultrasound as indicator of respiratory effort in critically ill patients undergoing assisted mechanical ventilation: a pilot clinical study.Crit Care. 2015 Apr 13;19(1):161. doi: 10.1186/s13054-015-0894-9. Crit Care. 2015. PMID: 25886857 Free PMC article.
-
Ultrasound assessment of ventilator-induced diaphragmatic dysfunction in mechanically ventilated pediatric patients.Paediatr Respir Rev. 2021 Dec;40:58-64. doi: 10.1016/j.prrv.2020.12.002. Epub 2021 Feb 23. Paediatr Respir Rev. 2021. PMID: 33744085 Review.
-
Advanced respiratory monitoring in mechanically ventilated patients with coronavirus disease 2019-associated acute respiratory distress syndrome.Curr Opin Crit Care. 2022 Feb 1;28(1):66-73. doi: 10.1097/MCC.0000000000000905. Curr Opin Crit Care. 2022. PMID: 34772836 Free PMC article. Review.
Cited by
-
Diaphragm Ultrasound in Different Clinical Scenarios: A Review with a Focus on Older Patients.Geriatrics (Basel). 2024 May 30;9(3):70. doi: 10.3390/geriatrics9030070. Geriatrics (Basel). 2024. PMID: 38920426 Free PMC article. Review.
-
Estimation of the transpulmonary pressure from the central venous pressure in mechanically ventilated patients.J Clin Monit Comput. 2024 Aug;38(4):847-858. doi: 10.1007/s10877-024-01150-5. Epub 2024 Mar 21. J Clin Monit Comput. 2024. PMID: 38512359 Free PMC article.
-
Clinical and Experimental Evidence for Patient Self-Inflicted Lung Injury (P-SILI) and Bedside Monitoring.J Clin Med. 2024 Jul 10;13(14):4018. doi: 10.3390/jcm13144018. J Clin Med. 2024. PMID: 39064059 Free PMC article. Review.
-
Assessing inspiratory drive and effort in critically ill patients at the bedside.Crit Care. 2025 Jul 31;29(1):339. doi: 10.1186/s13054-025-05526-0. Crit Care. 2025. PMID: 40745324 Free PMC article. Review.
-
Early Measurement of ROX Index in Intermediary Care Unit Is Associated with Mortality in Intubated COVID-19 Patients: A Retrospective Study.J Clin Med. 2022 Jan 12;11(2):365. doi: 10.3390/jcm11020365. J Clin Med. 2022. PMID: 35054058 Free PMC article.
References
-
- Grasselli G, Zangrillo A, Zanella A, Antonelli M, Cabrini L, Castelli A, Cereda D, Coluccello A, Foti G, Fumagalli R, Iotti G, Latronico N, Lorini L, Merler S, Natalini G, Piatti A, Ranieri MV, Scandroglio AM, Storti E, Cecconi M, Pesenti A, Network C-LI, Nailescu A, Corona A, Zangrillo A, Protti A, Albertin A, Forastieri Molinari A, Lombardo A, Pezzi A, Benini A, Scandroglio AM, Malara A, Castelli A, Coluccello A, Micucci A, Pesenti A, Sala A, Alborghetti A, Antonini B, Capra C, Troiano C, Roscitano C, Radrizzani D, Chiumello D, Coppini D, Guzzon D, Costantini E, Malpetti E, Zoia E, Catena E, Agosteo E, Barbara E, Beretta E, Boselli E, Storti E, Harizay F, Della Mura F, Lorini FL, Donato Sigurta F, Marino F, Mojoli F, Rasulo F, Grasselli G, Casella G, De Filippi G, Castelli G, Aldegheri G, Gallioli G, Lotti G, Albano G, Landoni G, Marino G, Vitale G, Battista Perego G, Evasi G, Citerio G, Foti G, Natalini G, Merli G, Sforzini I, Bianciardi L, Carnevale L, Grazioli L, Cabrini L, Guatteri L, Salvi L, Dei Poli M, Galletti M, Gemma M, Ranucci M, Riccio M, Borelli M, Zambon M, Subert M, Cecconi M, Mazzoni MG, Raimondi M, Panigada M, Belliato M, Bronzini N, Latronico N, Petrucci N, Belgiorno N, Tagliabue P, Cortellazzi P, Gnesin P, Grosso P, Gritti P, Perazzo P, Severgnini P, Ruggeri P, Sebastiano P, Covello RD, Fernandez-Olmos R, Fumagalli R, Keim R, Rona R, Valsecchi R, Cattaneo S, Colombo S, Cirri S, Bonazzi S, Greco S, Muttini S, Langer T, Alaimo V, Viola U. Baseline characteristics and outcomes of 1591 patients infected with SARS-CoV-2 admitted to ICUs of the Lombardy Region, Italy. JAMA. 2020;323:1574. - PMC - PubMed
-
- Wilcox SR. Management of respiratory failure due to covid-19. BMJ. 2020;369:m1786. - PubMed
-
- Marini JJ, Gattinoni L. Management of COVID-19 respiratory distress. JAMA. 2020;323:2329. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
