

The Interplay Between the Immune System, the Renin-Angiotensin-Aldosterone System (RAAS), and RAAS Inhibitors May Modulate the Outcome of COVID-19: A Systematic Review
- PMID: 33635546
- PMCID: PMC8014479
- DOI: 10.1002/jcph.1852
The Interplay Between the Immune System, the Renin-Angiotensin-Aldosterone System (RAAS), and RAAS Inhibitors May Modulate the Outcome of COVID-19: A Systematic Review
Abstract
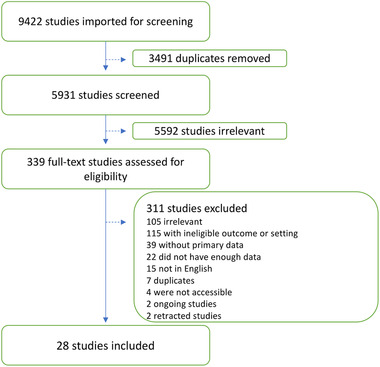
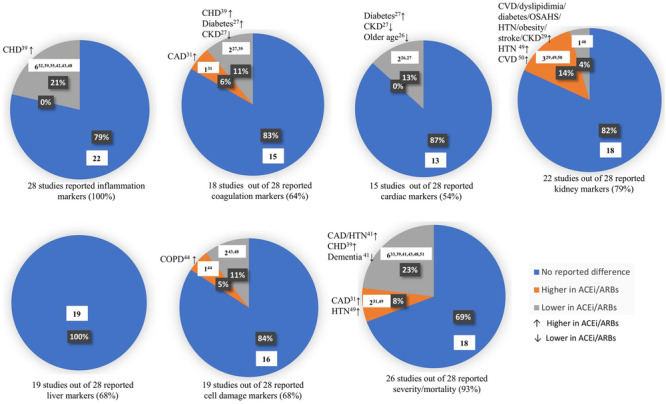
Since the discovery of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), numerous research has been undertaken to delineate the various effects of the virus which manifests in many ways all over the body. The association between the SARS-CoV-2 invasion mechanism and the renin-angiotensin-aldosterone system (RAAS) receptors, created many debates about the possible consequences of using RAAS-modulating drugs including angiotensin-converting enzyme inhibitors (ACEi) and angiotensin II receptor blockers (ARBs) during the pandemic. Many clinical studies were conducted to assess the outcomes of coronavirus disease 2019 (COVID-19) in patients who use ACEi/ARBs following the arguments claiming to discontinue these drugs as a precautionary measure. Although several studies mainly analyzed the outcomes of the disease, this review aimed to compare specific blood markers in both groups of COVID-19 patients to gain better insight into the interaction of ACEi/ARBs with different body functions during the infection. Several databases were searched using a combination of keywords followed by screening and data extraction. Only 28 studies met our inclusion criteria, the majority of which showed no significant difference between the inflammation markers of COVID-19 patients who used or did not use ACEi/ARBs. Interestingly, 6 studies reported lower inflammatory markers in COVID-19 patients who used ACEi/ARBs, and 6 studies reported better outcomes among the same group. We therefore concluded that the use of ACEi/ARBs may not lead to worse prognosis of COVID-19 and may even play a protective role against the hyperinflammatory response associated with COVID-19.
Keywords: Angiotensin-converting enzyme inhibitors; COVID-19; angiotensin receptor blockers; coronavirus; renin angiotensin aldosterone system.
© 2021, The American College of Clinical Pharmacology.
Conflict of interest statement
Mohamed B. Elshazly is a cofounder of EMBER Medical Telemedicine company, and he owns equity in this company, which is irrelevant to this research. The other authors declare no conflicts of interest.
Figures
References
-
- Johns Hopkins University . Johns Hopkins Coronavirus Resource Center. Johns Hopkins Coronavirus Resource Center. Baltimore, MD: Johns Hopkins University; 2020.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
