

Targeting RAGE to prevent SARS-CoV-2-mediated multiple organ failure: Hypotheses and perspectives
- PMID: 33636175
- PMCID: PMC7900755
- DOI: 10.1016/j.lfs.2021.119251
Targeting RAGE to prevent SARS-CoV-2-mediated multiple organ failure: Hypotheses and perspectives
Abstract
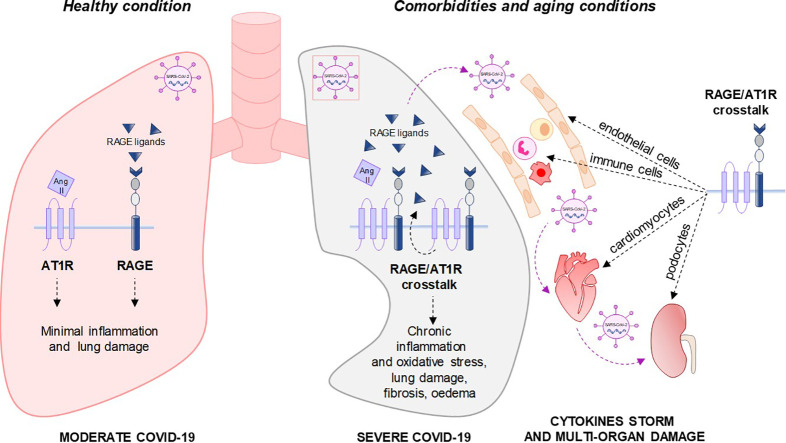
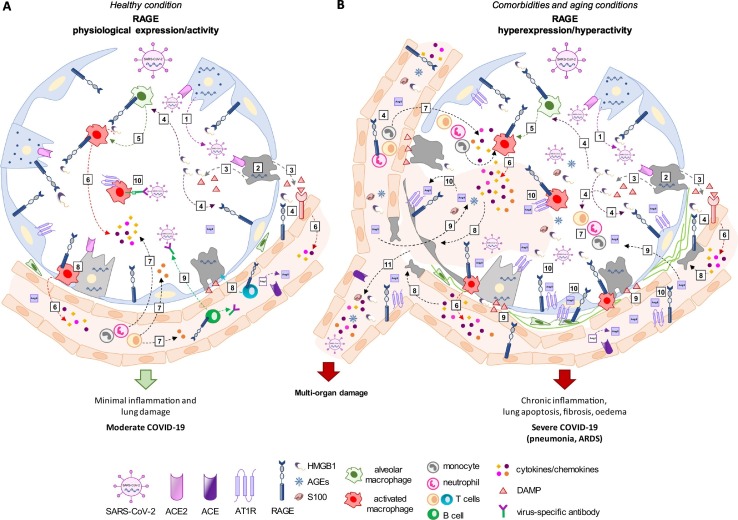
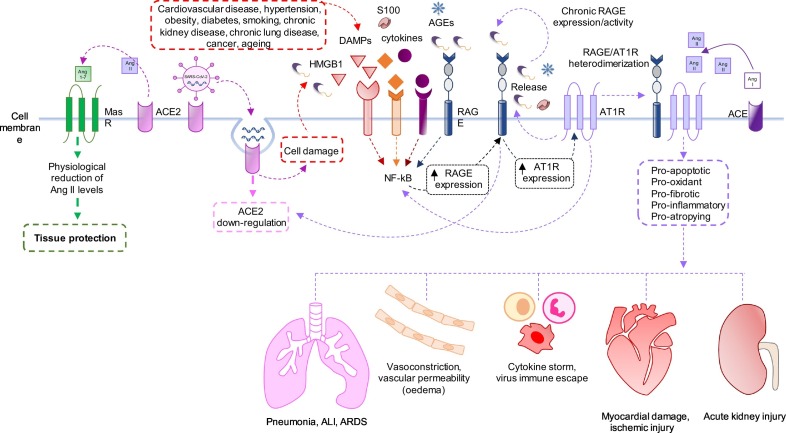
A novel infectious disease (COVID-19), caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), was detected in December 2019 and declared as a global pandemic by the World Health. Approximately 15% of patients with COVID-19 progress to severe pneumonia and eventually develop acute respiratory distress syndrome (ARDS), septic shock and/or multiple organ failure with high morbidity and mortality. Evidence points towards a determinant pathogenic role of members of the renin-angiotensin system (RAS) in mediating the susceptibility, infection, inflammatory response and parenchymal injury in lungs and other organs of COVID-19 patients. The receptor for advanced glycation end-products (RAGE), a member of the immunoglobulin superfamily, has important roles in pulmonary pathological states, including fibrosis, pneumonia and ARDS. RAGE overexpression/hyperactivation is essential to the deleterious effects of RAS in several pathological processes, including hypertension, chronic kidney and cardiovascular diseases, and diabetes, all of which are major comorbidities of SARS-CoV-2 infection. We propose RAGE as an additional molecular target in COVID-19 patients for ameliorating the multi-organ pathology induced by the virus and improving survival, also in the perspective of future infections by other coronaviruses.
Keywords: COVID-19; HMGB1; RAGE; Renin-angiotensin system (RAS); SARS-CoV-2.
Copyright © 2021 Elsevier Inc. All rights reserved.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Similar articles
-
Hyperactivated RAGE in Comorbidities as a Risk Factor for Severe COVID-19-The Role of RAGE-RAS Crosstalk.Biomolecules. 2021 Jun 12;11(6):876. doi: 10.3390/biom11060876. Biomolecules. 2021. PMID: 34204735 Free PMC article. Review.
-
Impairing RAGE signaling promotes survival and limits disease pathogenesis following SARS-CoV-2 infection in mice.JCI Insight. 2022 Jan 25;7(2):e155896. doi: 10.1172/jci.insight.155896. JCI Insight. 2022. PMID: 35076028 Free PMC article.
-
Receptor for advanced glycation end-products axis and coronavirus disease 2019 in inflammatory bowel diseases: A dangerous liaison?World J Gastroenterol. 2021 May 21;27(19):2270-2280. doi: 10.3748/wjg.v27.i19.2270. World J Gastroenterol. 2021. PMID: 34040321 Free PMC article. Review.
-
Testing the efficacy and safety of BIO101, for the prevention of respiratory deterioration, in patients with COVID-19 pneumonia (COVA study): a structured summary of a study protocol for a randomised controlled trial.Trials. 2021 Jan 11;22(1):42. doi: 10.1186/s13063-020-04998-5. Trials. 2021. PMID: 33430924 Free PMC article.
-
Drugs acting on the renin-angiotensin system and SARS-CoV-2.Drug Discov Today. 2021 Apr;26(4):870-874. doi: 10.1016/j.drudis.2021.01.010. Epub 2021 Jan 21. Drug Discov Today. 2021. PMID: 33486116 Free PMC article. Review.
Cited by
-
Consequences of COVID-19 for the Pancreas.Int J Mol Sci. 2022 Jan 13;23(2):864. doi: 10.3390/ijms23020864. Int J Mol Sci. 2022. PMID: 35055050 Free PMC article. Review.
-
Hyperactivated RAGE in Comorbidities as a Risk Factor for Severe COVID-19-The Role of RAGE-RAS Crosstalk.Biomolecules. 2021 Jun 12;11(6):876. doi: 10.3390/biom11060876. Biomolecules. 2021. PMID: 34204735 Free PMC article. Review.
-
Age, obesity and hyperglycaemia: Activation of innate immunity initiates a series of molecular interactions involving anionic surfaces leading to COVID-19 morbidity and mortality.Med Hypotheses. 2021 Oct;155:110646. doi: 10.1016/j.mehy.2021.110646. Epub 2021 Aug 3. Med Hypotheses. 2021. PMID: 34392108 Free PMC article.
-
Advanced glycation end products (AGEs) and its receptor, RAGE, modulate age-dependent COVID-19 morbidity and mortality. A review and hypothesis.Int Immunopharmacol. 2021 Sep;98:107806. doi: 10.1016/j.intimp.2021.107806. Epub 2021 May 24. Int Immunopharmacol. 2021. PMID: 34352471 Free PMC article. Review.
-
Serum Albumin in Health and Disease: Esterase, Antioxidant, Transporting and Signaling Properties.Int J Mol Sci. 2021 Sep 25;22(19):10318. doi: 10.3390/ijms221910318. Int J Mol Sci. 2021. PMID: 34638659 Free PMC article. Review.
References
-
- Ge X.Y., Li J.L., Yang X.L., Chmura A.A., Zhu G., Epstein J.H., Mazet J.K., Hu B., Zhang W., Peng C., Zhang Y.J., Luo C.M., Tan B., Wang N., Zhu Y., Crameri G., Zhang S.Y., Wang L.F., Daszak P., Shi Z.L. Isolation and characterization of a bat SARS-like coronavirus that uses the ACE2 receptor. Nature. 2013;503:535–538. doi: 10.1038/nature12711. - DOI - PMC - PubMed
-
- Huang C., Wang Y., Li X., Ren L., Zhao J., Hu Y., Zhang L., Fan G., Xu J., Gu X., Cheng Z., Yu T., Xia J., Wei Y., Wu W., Xie X., Yin W., Li H., Liu M., Xiao Y., Gao H., Guo L., Xie J., Wang G., Jiang R., Gao Z., Jin Q., Wang J., Cao B. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China [published correction appears in Lancet. 2020 Jan 30] Lancet. 2020;395:497–506. doi: 10.1016/S0140-6736(20)30183-5. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
