

Gliosarcoma in patients under 20 years of age. A clinicopathologic study of 11 cases and detailed review of the literature
- PMID: 33637068
- PMCID: PMC7908689
- DOI: 10.1186/s12887-021-02556-9
Gliosarcoma in patients under 20 years of age. A clinicopathologic study of 11 cases and detailed review of the literature
Abstract
Background: Gliosarcoma is a rare variant of IDH- wild type glioblastoma with both glial and mesenchymal differentiation. It accounts for approximately 2% of glioblastomas and has a poor prognosis similar to that of classic glioblastoma. It is seen mostly between 40 and 60 years of age with a mean age over 50 years. Pediatric gliosarcoma is even rarer than gliosarcoma in adults. We describe the clinicopathological features of gliosarcoma in patients under 20 years of age and determine whether there are significant differences from gliosarcoma in adults. We also present detailed review of published literature on pediatric gliosarcoma.
Methods: Slides of gliosarcomas in patients under 20 years of age were reviewed. Clinicopathological features were noted in detail and follow up was obtained.
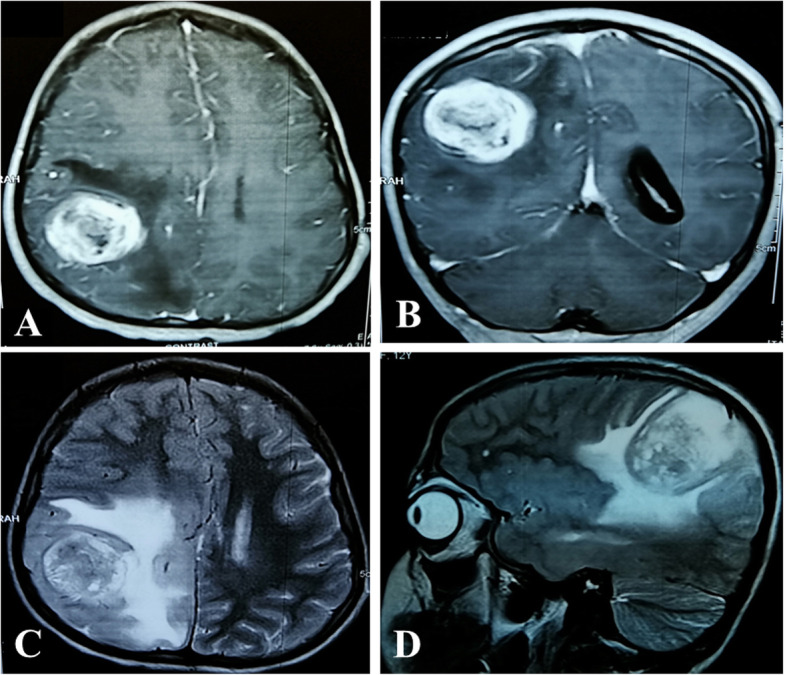
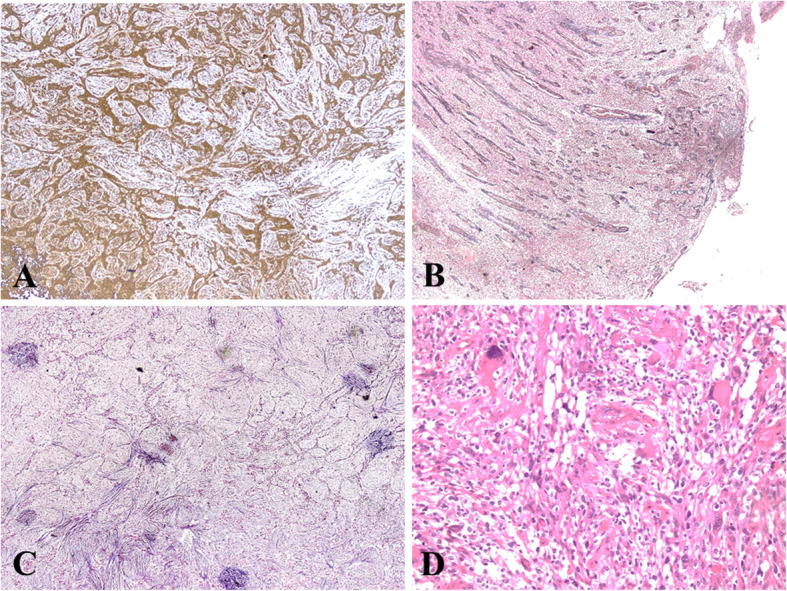
Results: Eleven cases of gliosarcoma were reported in patients under 20 years of age. Ages ranged from three to 19 years (mean age 13 years). Frontal, parietal and temporal lobes were the commonest locations. Mean and median tumor size was six and five cm respectively. All 11 cases demonstrated the classic biphasic pattern. In 10 cases, glial component was astrocytic and was highlighted on GFAP. Sarcomatous component in most cases resembled fibrosarcoma and was high grade in 72.7%. Glial areas were reticulin poor while sarcomatous areas were reticulin rich. In over 45% cases, bizarre tumor giant cells were seen in the sarcomatous areas. In 1 case, sarcomatous areas showed extensive bone and cartilage formation. Other histologic features included hyalinized blood vessels, hemorrhage, infarction, gemistocytic cells, rhabdoid cells etc. Follow up was available in nine patients, five received chemoradiation post resection while three received radiotherapy only. Prognosis was dismal and eight patients died within one to 14 months following resection.
Conclusions: Gliosarcomas in patients under 20 comprised 13% of all gliosarcomas reported during the study period. Frequency and mean age were higher compared to other published reports. Pathological features were similar to those described in literature. Clinicopathological features and prognosis of pediatric gliosarcomas were similar to adult gliosarcomas.
Keywords: Astrocytic; Biphasic; Cerebral hemispheres; Glial; Glioblastoma; Gliosarcoma; Mesenchymal; Pediatric.
Conflict of interest statement
It is declared that all authors have no conflict of interest.
Figures


References
-
- Burger PC, Giangaspero F, Ohgaki H, Bieruat W, et al. Gliosarcoma. In: Louis DN, Ohgaki H, WK WODC, Ellison DW, Figarella–Branger D, Perry A, et al., editors. WHO Classification of Tumours of the Central Nervous System. Revised 4th Edition. International Agency for Research on Cancer (IARC) Lyon. 2016. pp. 48–49.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
