

TGFβ1 neutralization displays therapeutic efficacy through both an immunomodulatory and a non-immune tumor-intrinsic mechanism
- PMID: 33637600
- PMCID: PMC7919595
- DOI: 10.1136/jitc-2020-001798
TGFβ1 neutralization displays therapeutic efficacy through both an immunomodulatory and a non-immune tumor-intrinsic mechanism
Abstract
Background: Transforming growth factor-β (TGFβ) is emerging as a promising target for cancer therapy, given its ability to promote progression of advanced tumors and to suppress anti-tumor immune responses. However, TGFβ also plays multiple roles in normal tissues, particularly during organogenesis, raising toxicity concerns about TGFβ blockade. Dose-limiting cardiovascular toxicity was observed, possibly due to the blockade of all three TGFβ isoforms. The dominant isoform in tumors is TGFβ1, while TGFβ2 and TGFβ3 seem to be more involved in cardiovascular development. Recent data indicated that selective targeting of TGFβ1 promoted the efficacy of checkpoint inhibitor anti-PD1 in transplanted preclinical tumor models, without cardiovascular toxicity.
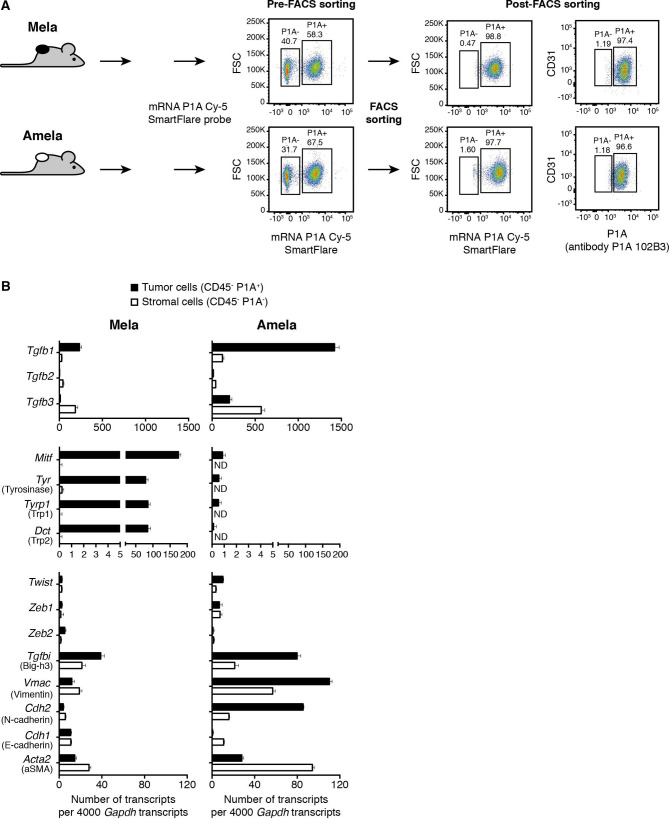
Methods: To further explore the therapeutic potential of isoform-specific TGFβ blockade, we developed neutralizing mAbs targeting mature TGFβ1 or TGFβ3, and tested them, in parallel with anti-panTGFβ mAb 1D11, in two preclinical models: the transplanted colon cancer model CT26, and the autochthonous melanoma model TiRP.
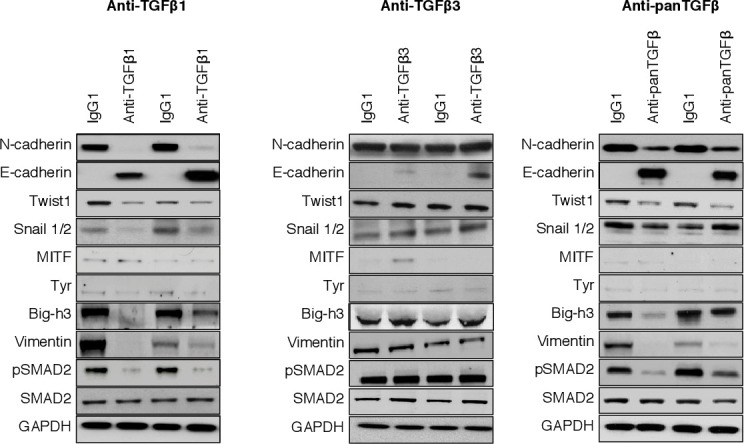
Results: We observed that the blockade of TGFβ1, but not that of TGFβ3, increased the efficacy of a prophylactic cellular vaccine against colon cancer CT26. This effect was similar to pan-TGFβ blockade, and was associated with increased infiltration of activated CD8 T cells in the tumor, and reduced levels of regulatory T cells and myeloid-derived suppressor cells. In contrast, in the autochthonous TiRP melanoma model, we observed therapeutic efficacy of the TGFβ1-specific mAb as a single agent, while the TGFβ3 mAb was inactive. In this model, the anti-tumor effect of TGFβ1 blockade was tumor intrinsic rather than immune mediated, as it was also observed in T-cell depleted mice. Mechanistically, TGFβ1 blockade increased mouse survival by delaying the phenotype switch, akin to epithelial-to-mesenchymal transition (EMT), which transforms initially pigmented tumors into highly aggressive unpigmented tumors.
Conclusions: Our results confirm TGFβ1 as the relevant isoform to target for cancer therapy, not only in combination with checkpoint inhibitors, but also with other immunotherapies such as cancer vaccines. Moreover, TGFβ1 blockade can also act as a monotherapy, through a tumor-intrinsic effect blocking the EMT-like transition. Because human melanomas that resist therapy often express a gene signature that links TGFβ1 with EMT-related genes, these results support the clinical development of TGFβ1-specific mAbs in melanoma.
Keywords: cytokines; drug evaluation; immunomodulation; immunotherapy; melanoma; preclinical.
© Author(s) (or their employer(s)) 2021. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: BJVdE is co-founder of, has ownership interest in, and is SAB member of iTeos Therapeutics.
Figures



Similar articles
-
Dual inhibition of TGFβ2,3 is severely toxic, whereas selective inhibition of TGFβ1, 2, or 3 and dual inhibition of TGFβ1,2 is generally tolerated in mouse and cynomolgus monkey toxicology studies.Toxicol Sci. 2025 Aug 1;206(2):445-455. doi: 10.1093/toxsci/kfaf059. Toxicol Sci. 2025. PMID: 40317126
-
Progression of melanoma is suppressed by targeting all transforming growth factor‑β isoforms with an Fc chimeric receptor.Oncol Rep. 2021 Sep;46(3):197. doi: 10.3892/or.2021.8148. Epub 2021 Jul 23. Oncol Rep. 2021. PMID: 34296292 Free PMC article.
-
Targeting the vascular endothelial growth factor receptor-1 by the monoclonal antibody D16F7 to increase the activity of immune checkpoint inhibitors against cutaneous melanoma.Pharmacol Res. 2020 Sep;159:104957. doi: 10.1016/j.phrs.2020.104957. Epub 2020 May 30. Pharmacol Res. 2020. PMID: 32485280
-
Curing tumor-bearing mice by shifting a Th2 to a Th1 anti-tumor response.Hum Antibodies. 2017;25(3-4):147-153. doi: 10.3233/HAB-160309. Hum Antibodies. 2017. PMID: 28085017 Review.
-
The role of integrins in TGFβ activation in the tumour stroma.Cell Tissue Res. 2016 Sep;365(3):657-73. doi: 10.1007/s00441-016-2474-y. Epub 2016 Aug 12. Cell Tissue Res. 2016. PMID: 27515461 Free PMC article. Review.
Cited by
-
Inhibition of PCSK9 enhances the antitumor effect of PD-1 inhibitor in colorectal cancer by promoting the infiltration of CD8+ T cells and the exclusion of Treg cells.Front Immunol. 2022 Aug 8;13:947756. doi: 10.3389/fimmu.2022.947756. eCollection 2022. Front Immunol. 2022. PMID: 36003387 Free PMC article.
-
Regulation of T cells by myeloid-derived suppressor cells: emerging immunosuppressor in lung cancer.Discov Oncol. 2023 Oct 19;14(1):185. doi: 10.1007/s12672-023-00793-1. Discov Oncol. 2023. PMID: 37857728 Free PMC article. Review.
-
Pan-cancer analysis suggests histocompatibility minor 13 is an unfavorable prognostic biomarker promoting cell proliferation, migration, and invasion in hepatocellular carcinoma.Front Pharmacol. 2022 Aug 15;13:950156. doi: 10.3389/fphar.2022.950156. eCollection 2022. Front Pharmacol. 2022. PMID: 36046831 Free PMC article.
-
Platelets in cancer and immunotherapy: functional dynamics and therapeutic opportunities.Exp Hematol Oncol. 2025 Jun 13;14(1):83. doi: 10.1186/s40164-025-00676-x. Exp Hematol Oncol. 2025. PMID: 40514754 Free PMC article. Review.
-
The enhanced antitumor activity of bispecific antibody targeting PD-1/PD-L1 signaling.Cell Commun Signal. 2024 Mar 12;22(1):179. doi: 10.1186/s12964-024-01562-5. Cell Commun Signal. 2024. PMID: 38475778 Free PMC article. Review.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials