

Expression of p53 is significantly associated with recurrence-free survival and overall survival in pleuropulmonary blastoma (PPB): a report from the International Pleuropulmonary Blastoma/DICER1 Registry
- PMID: 33637876
- PMCID: PMC9236228
- DOI: 10.1038/s41379-021-00735-8
Expression of p53 is significantly associated with recurrence-free survival and overall survival in pleuropulmonary blastoma (PPB): a report from the International Pleuropulmonary Blastoma/DICER1 Registry
Abstract
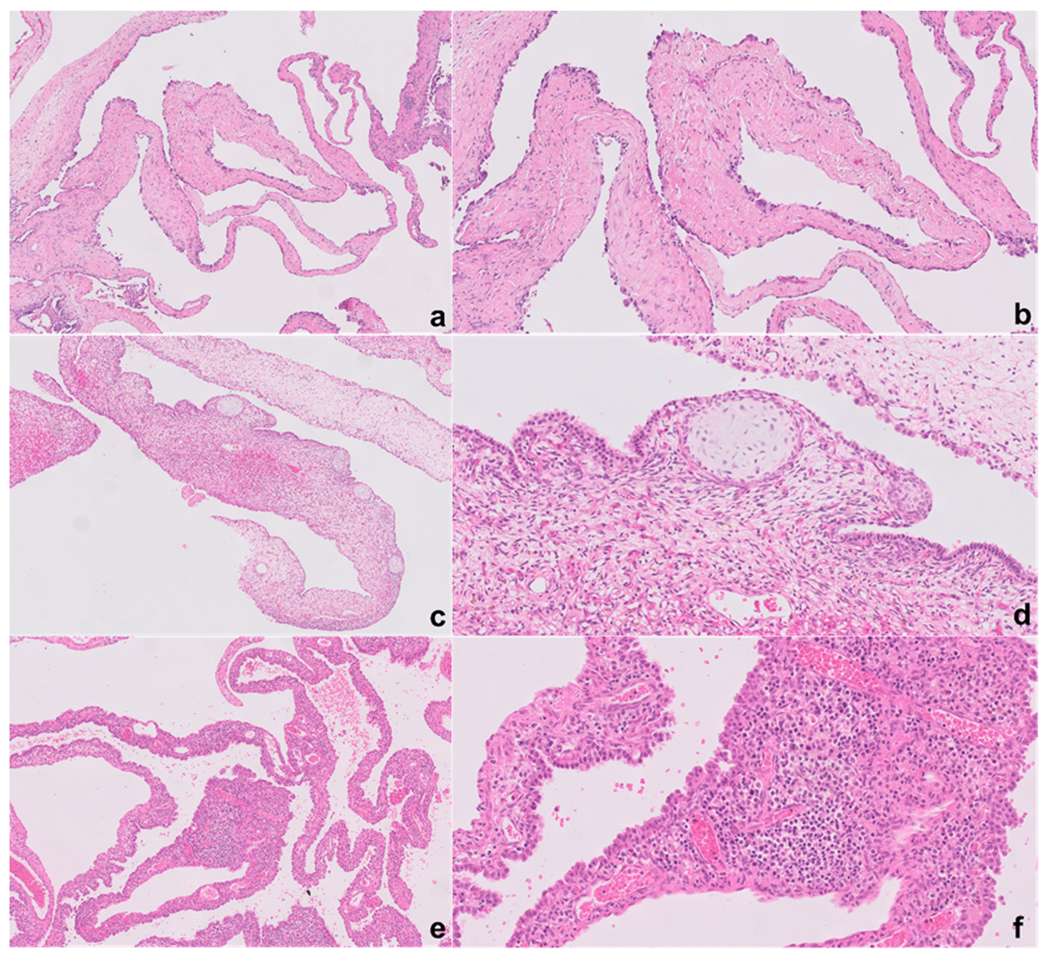
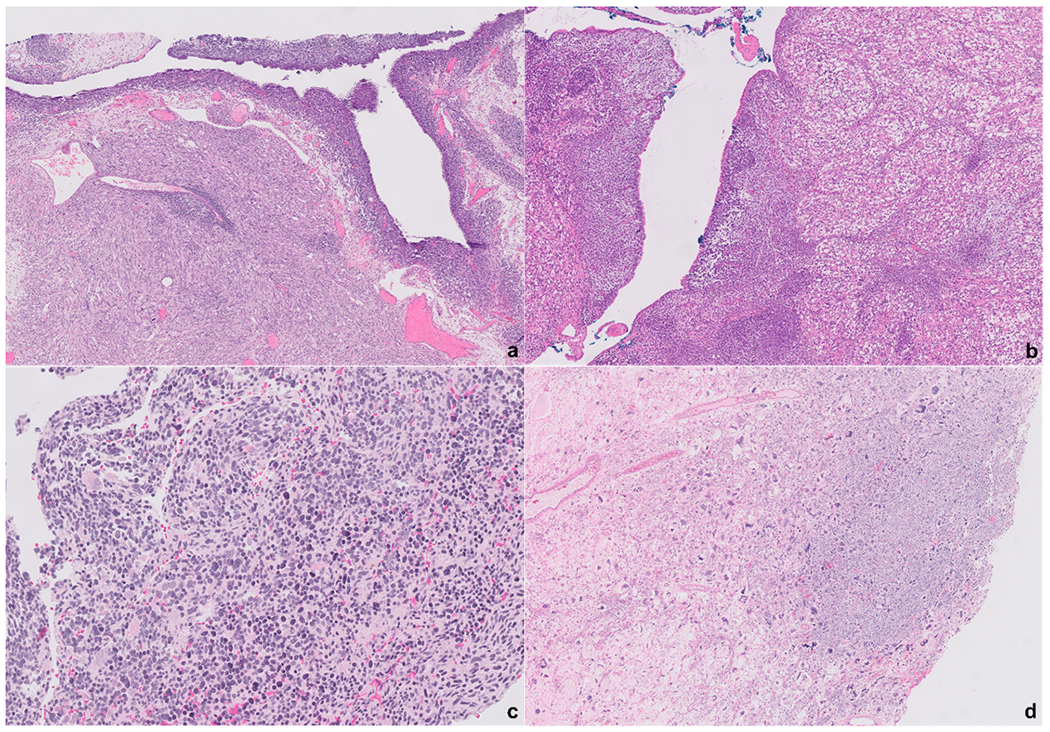
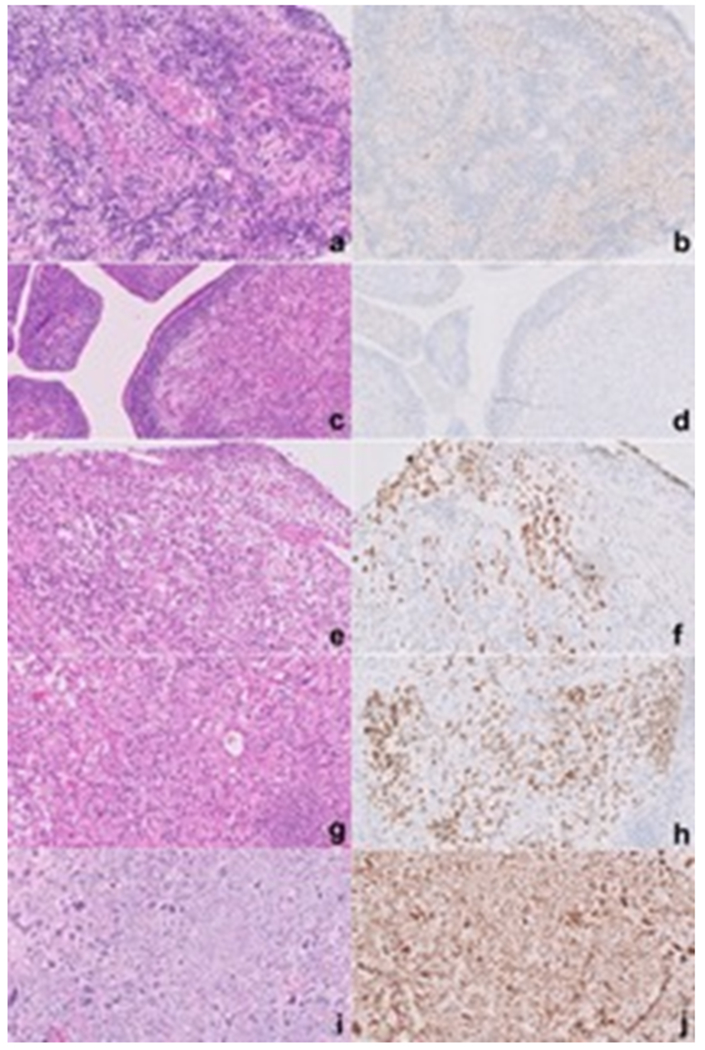
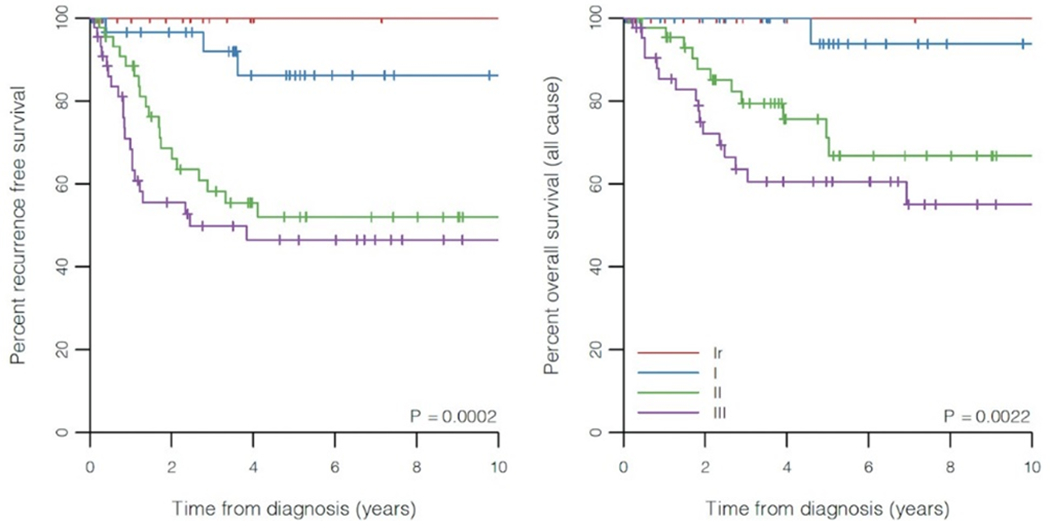
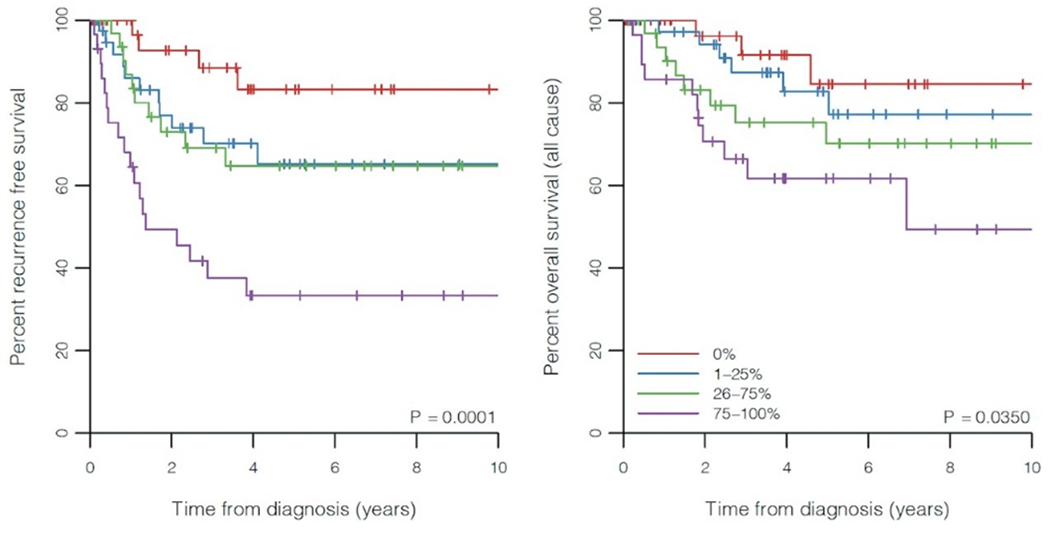
Pleuropulmonary blastoma (PPB) is a primary embryonal malignancy of childhood that is characterized by distinct morphologic types: type Ir (regressed), type I (cystic), type II (cystic and solid), and type III (solid). Prognosis varies by PPB type. Most cases are associated with a germline pathogenic mutation in DICER1; however, there is limited data on the factor(s) at a cellular level that drive progression from type I to type III. In this study, we evaluated the expression of p53 and its prognostic implications. A total of 143 PPB cases were included in the study with the following distribution in PPB types: Ir (14%), I (23%), II (32%), and III (31%). P53 expression by immunohistochemistry (IHC) was recorded as four groups: 0%, 1-25%, 26-75%, and 76-100%. All type I PPBs showed 0-25% p53 expression compared to the higher p53 expression (>25%) in type III PPB (p < 0.0001), to support the argument that p53 has a role in tumor progression. In addition, type Ir with the architectural hallmarks of type I PPB, but lacking the primitive cell population, has negligible p53 expression. High p53 expression (staining observed in >25% of the tumor cells) was significantly associated with age over 1 year (p = 0.0033), neoadjuvant therapy (p = 0.0009), positive resection margin (p = 0.0008) and anaplasia (p < 0.0001). P53 expression was significantly associated with recurrence-free survival (p < 0.0001) and overall survival (p = 0.0350), with higher p53 expression associated with worse prognosis. Comparisons of concordance statistics showed no significant difference in prognostication when using morphologic types compared to p53 expression groups (p = 0.647). TP53 sequence was performed in 16 cases; the most common variant identified was a missense variant (12 cases), and in one case a frameshift truncating variant was noted. Based on these findings, we recommend performing p53 IHC in all newly diagnosed cases of types II and III PPB to further aid in risk stratification.
Conflict of interest statement
Disclosure
D. Ashley Hill is the owner of ResourcePath, a private research and clinical laboratory. ResourcePath has no financial interests or products described in or promoted by this manuscript.
Figures

Similar articles
-
Pleuropulmonary blastoma: a report on 350 central pathology-confirmed pleuropulmonary blastoma cases by the International Pleuropulmonary Blastoma Registry.Cancer. 2015 Jan 15;121(2):276-85. doi: 10.1002/cncr.29032. Epub 2014 Sep 10. Cancer. 2015. PMID: 25209242 Free PMC article.
-
Health-related quality of life in children and adolescents with pleuropulmonary blastoma: A report from the International PPB/DICER1 Registry.Pediatr Blood Cancer. 2023 Apr;70(4):e30077. doi: 10.1002/pbc.30077. Epub 2022 Nov 24. Pediatr Blood Cancer. 2023. PMID: 36424733 Free PMC article.
-
Type II Pleuropulmonary Blastoma in a 4 Month Old Infant with Negative Dicer1 Mutation on Next Generation Sequencing.Med Arch. 2021 Feb;75(1):61-65. doi: 10.5455/medarh.2021.75.61-65. Med Arch. 2021. PMID: 34012202 Free PMC article.
-
Type I pleuropulmonary blastoma: pathology and biology study of 51 cases from the international pleuropulmonary blastoma registry.Am J Surg Pathol. 2008 Feb;32(2):282-95. doi: 10.1097/PAS.0b013e3181484165. Am J Surg Pathol. 2008. PMID: 18223332 Review.
-
Cerebral metastasis and other central nervous system complications of pleuropulmonary blastoma.Pediatr Blood Cancer. 2007 Sep;49(3):266-73. doi: 10.1002/pbc.20937. Pediatr Blood Cancer. 2007. PMID: 16807914 Review.
Cited by
-
Expanding Our Knowledge of DICER1 Gene Alterations and Their Role in Thyroid Diseases.Cancers (Basel). 2024 Jan 13;16(2):347. doi: 10.3390/cancers16020347. Cancers (Basel). 2024. PMID: 38254836 Free PMC article. Review.
-
DICER1 Syndrome: A Multicenter Surgical Experience and Systematic Review.Cancers (Basel). 2023 Jul 19;15(14):3681. doi: 10.3390/cancers15143681. Cancers (Basel). 2023. PMID: 37509342 Free PMC article.
-
Pleuropulmonary Blastoma: A Report of Two Rare Cases.Cureus. 2024 May 10;16(5):e60021. doi: 10.7759/cureus.60021. eCollection 2024 May. Cureus. 2024. PMID: 38854270 Free PMC article.
-
GPC3: a novel mutated gene in pleuropulmonary blastoma.Discov Oncol. 2025 Jul 16;16(1):1350. doi: 10.1007/s12672-025-02937-x. Discov Oncol. 2025. PMID: 40670689 Free PMC article.
-
DICER1 tumor predisposition syndrome: an evolving story initiated with the pleuropulmonary blastoma.Mod Pathol. 2022 Jan;35(1):4-22. doi: 10.1038/s41379-021-00905-8. Epub 2021 Oct 1. Mod Pathol. 2022. PMID: 34599283 Free PMC article. Review.
References
-
- Manivel JC, Priest JR, Watterson J, Steiner M, Woods WG, Wick MR, et al. Pleuropulmonay Blastoma. The So-Called Pulmonary Blastoma of Childhood. Cancer. 1988;62:1516–26. - PubMed
-
- Dehner LP. Pleuropulmonary Blastoma is THE Pulmonary Blastoma of Childhood. Semin Diagn Pathol. 1994;11:144–51. - PubMed
-
- Priest JR, Watterson J, Strong L, Huff V, Woods WG, Byrd RL, et al. Pleuropulmonary blastoma: A marker for familial disease. J Pediatr. 1996;128:220–4. - PubMed
-
- Schultz KAP, Stewart DR, Kamihara J, Bauer AJ, Merideth MA, Stratton P, et al. DICER1 Tumor Predisposition. In: Adam MP, Ardinger HH, Pagon RA, Wallace SE, Bean LJH, Stephens K, et al., editors. Seattle (WA); 2014.
Publication types
MeSH terms
Substances
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
