

Bariatric-Metabolic Surgery Utilisation in Patients With and Without Diabetes: Data from the IFSO Global Registry 2015-2018
- PMID: 33638756
- PMCID: PMC8113173
- DOI: 10.1007/s11695-021-05280-6
Bariatric-Metabolic Surgery Utilisation in Patients With and Without Diabetes: Data from the IFSO Global Registry 2015-2018
Abstract
Background: Comparative international practice of patients undergoing bariatric-metabolic surgery for type 2 diabetes mellitus (T2DM) is unknown. We aimed to ascertain baseline age, sex, body mass index (BMI) and types of operations performed for patients with T2DM submitted to the IFSO Global Registry.
Materials and methods: Cross-sectional analysis of patients having primary surgery in 2015-2018 for countries with ≥90% T2DM data completion and ≥ 1000 submitted records.
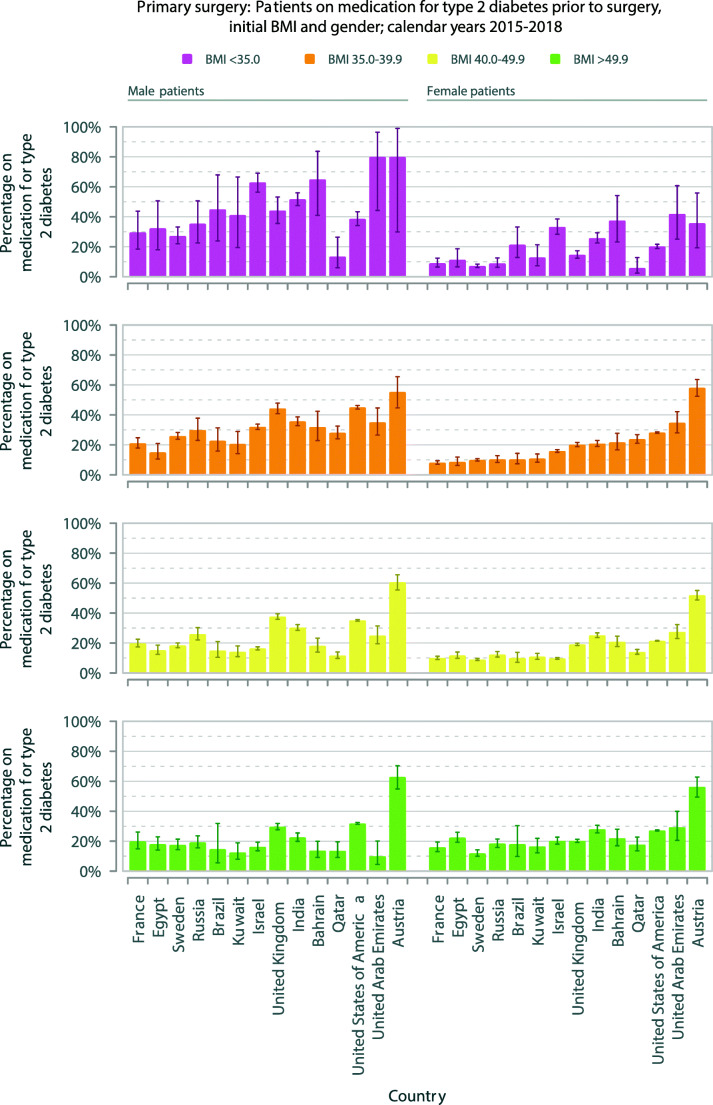
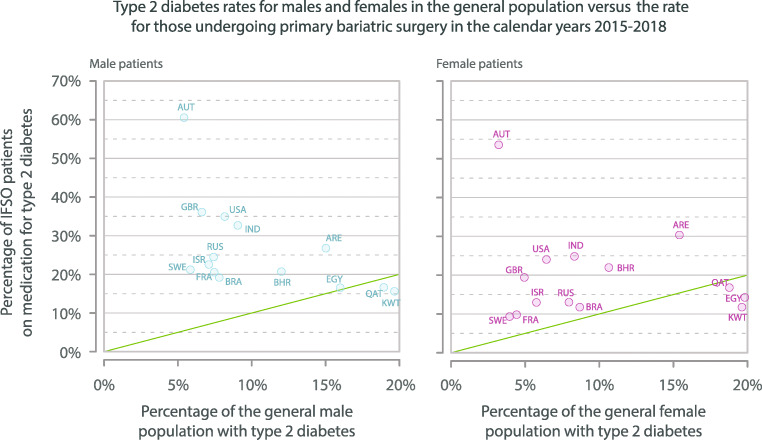
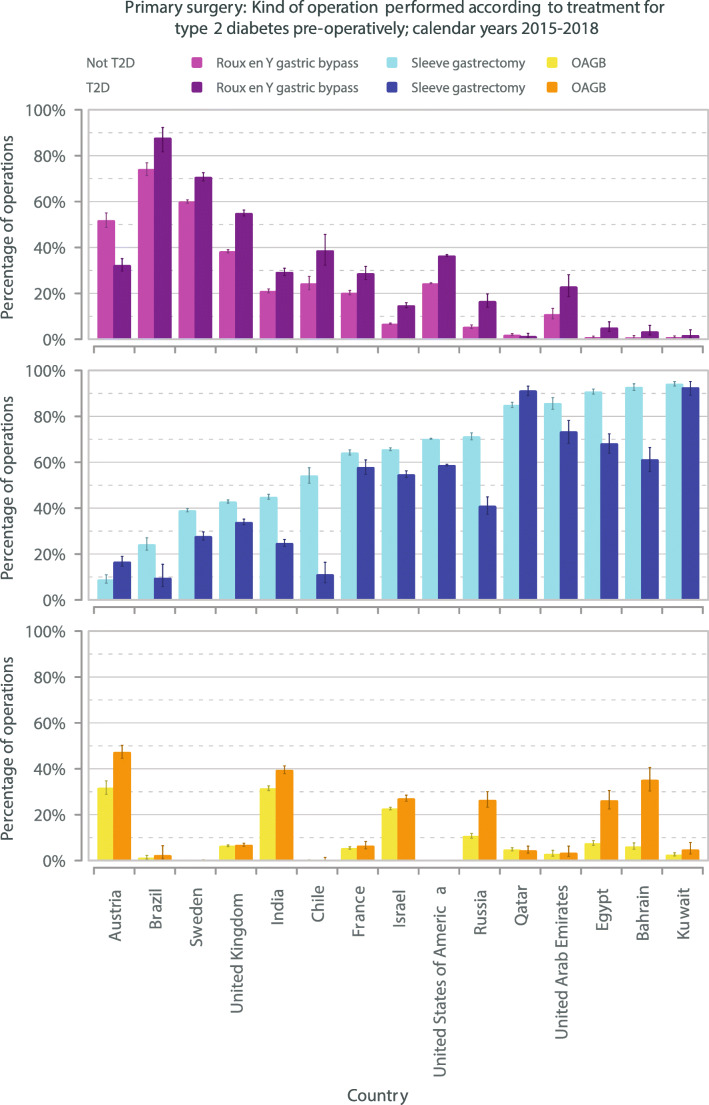
Results: Fifteen countries including 11 national registries met the inclusion criteria. The rate of T2DM was 24.2% (99,537 of 411,581 patients, country range 12.0-55.1%) and 77.1% of all patients were women. In every country, patients with T2DM were older than those without T2DM (overall mean age 49.2 [SD 11.4] years vs 41.8 [11.9] years, all p < 0.001). Men were more likely to have T2DM than women, odds ratio (OR) 1.68 (95% CI 1.65-1.71), p < 0.001. Men showed higher rates of T2DM for BMI <35 kg/m2 compared to BMI ≥35.0 kg/m2, OR 2.76 (2.52-3.03), p < 0.001. This was not seen in women, OR 0.78 (0.73-0.83), p < 0.001. Sleeve gastrectomy was the commonest operation overall, but less frequent for patients with T2DM, patients with T2DM 54.9% vs without T2DM 65.8%, OR 0.63 (0.63-0.64), p < 0.001. Twelve out of 15 countries had higher proportions of gastric bypass compared to non-bypass operations for T2DM, OR 1.70 (1.67-1.72), p < 0.001.
Conclusion: Patients with T2DM had different characteristics to those without T2DM. Older men were more likely to have T2DM, with higher rates of BMI <35 kg/m2 and increased likelihood of food rerouting operations.
Keywords: Bariatric surgery; Comorbidity; Demographic classification; IFSO Global Registry; Metabolic surgery; Obesity surgery; Operation choice for diabetes; Sex characteristics; Type 2 diabetes.
Conflict of interest statement
Dr Welbourn reports personal fees from Novo Nordisk, outside the submitted work.
Drs Kinsman and Walton report grants from IFSO, outside the submitted work.
Dr Dixon reports personal fees from NHMRC, during the conduct of the study; personal fees from Reshape, personal fees from Bariatric Advantage, personal fees from Novo Nordisk, personal fees from Nestle Health Science, personal fees from Johnson & Johnson, and personal feed from I-Nova, outside the submitted work.
Dr Cohen reports personal fees from GI Dynamics, grants from Johnson & Johnson Medical, Brazil, outside the submitted work.
Dr Ottosson reports consultancy fees from Johnson & Johnson and Vifor Pharma, outside the submitted work.
Dr Anvari reports consultancy fees from Johnson & Johnson, outside the submitted work.
Dr Himpens reports personal fees from Ethicon, personal fees from Medtronic, outside the submitted work.
Dr Brown reports grants from Johnson and Johnson, grants from Medtronic, grants from GORE, personal fees from GORE, grants from Applied Medical, grants from Apollo Endosurgery, grants and personal fees from Novo Nordisk, personal fees from Merck Sharpe and Dohme, outside the submitted work; and I am a bariatric surgeon so earn my living from performing these procedures.
Drs Hollyman, Morton, Ghaferi, Higa, Pattou, Al-Sabah, Liem, Våge, Kow have nothing to disclose.
Figures
Comment in
-
The Need for Better Clarification Regarding Hiatal Hernia Observed During Bariatric Surgery.Obes Surg. 2023 Feb;33(2):670-671. doi: 10.1007/s11695-022-06393-2. Epub 2022 Dec 11. Obes Surg. 2023. PMID: 36502437 No abstract available.
References
-
- Hofsø D, Fatima F, Borgeraas H, et al. Gastric bypass versus sleeve gastrectomy in patients with type 2 diabetes (Oseberg): a singlecenter, triple-blind, randomized controlled trial. Lancet Diabetes Endocrinol. 2019;7(12):912–24. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
