

Decentralisation, integration, and task-shifting in hepatitis C virus infection testing and treatment: a global systematic review and meta-analysis
- PMID: 33639097
- PMCID: PMC7966682
- DOI: 10.1016/S2214-109X(20)30505-2
Decentralisation, integration, and task-shifting in hepatitis C virus infection testing and treatment: a global systematic review and meta-analysis
Abstract
Background: Increasing access to hepatitis C virus (HCV) care and treatment will require simplified service delivery models. We aimed to evaluate the effects of decentralisation and integration of testing, care, and treatment with harm-reduction and other services, and task-shifting to non-specialists on outcomes across the HCV care continuum.
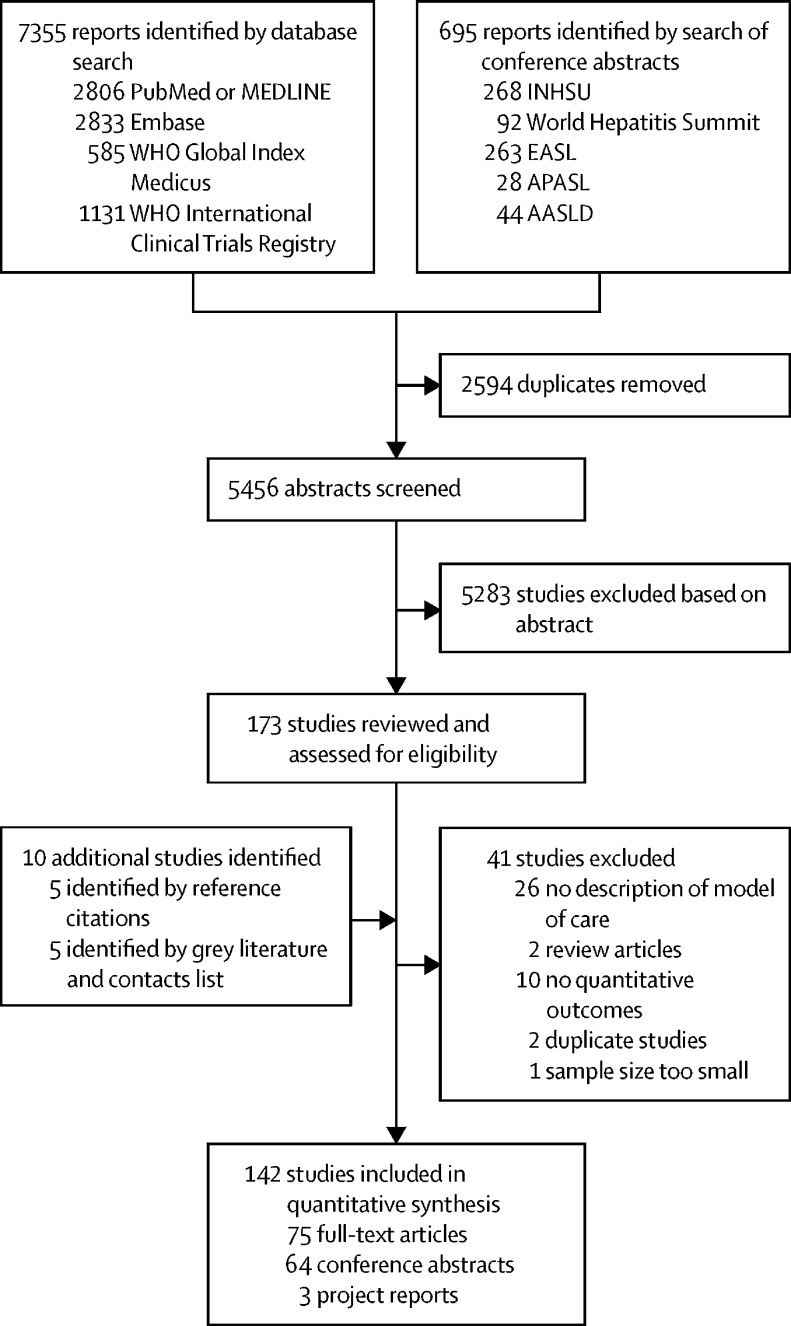
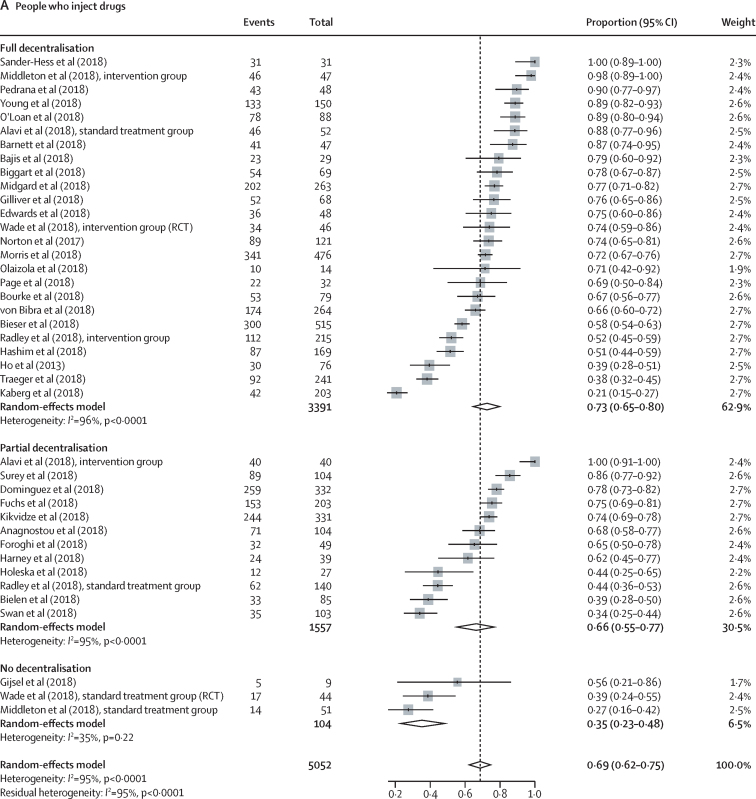
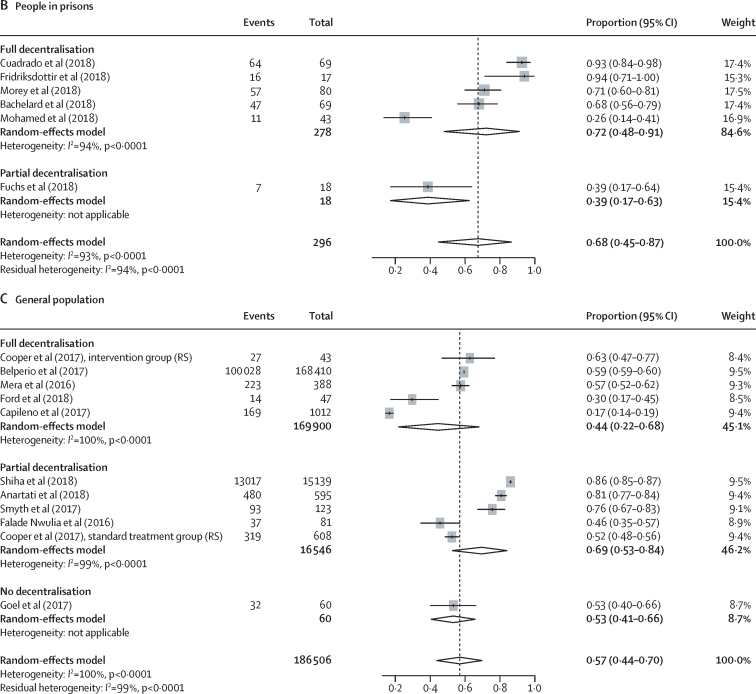
Methods: For this systematic review and meta-analysis, we searched PubMed, Embase, WHO Global Index Medicus, and conference abstracts for studies published between Jan 1, 2008, and Feb 20, 2018, that evaluated uptake of HCV testing, linkage to care, treatment, cure assessment, and sustained virological response at 12 weeks (SVR12) in people who inject drugs, people in prisons, people living with HIV, and the general population. Randomised controlled trials, non-randomised studies, and observational studies were eligible for inclusion. Studies with a sample size of ten or less for the largest denominator were excluded. Studies were categorised according to the level of decentralisation: full (testing and treatment at same site), partial (testing at decentralised site and referral elsewhere for treatment), or none. Task-shifting was categorised as treatment by specialists or non-specialists. Data on outcomes across the HCV care continuum (linkage to care, treatment uptake, and SVR12) were pooled using random-effects meta-analysis.
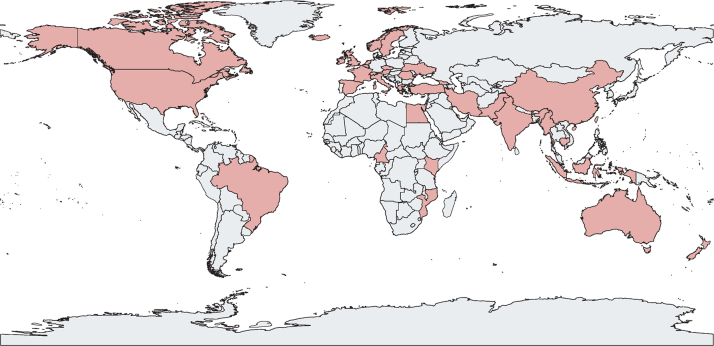
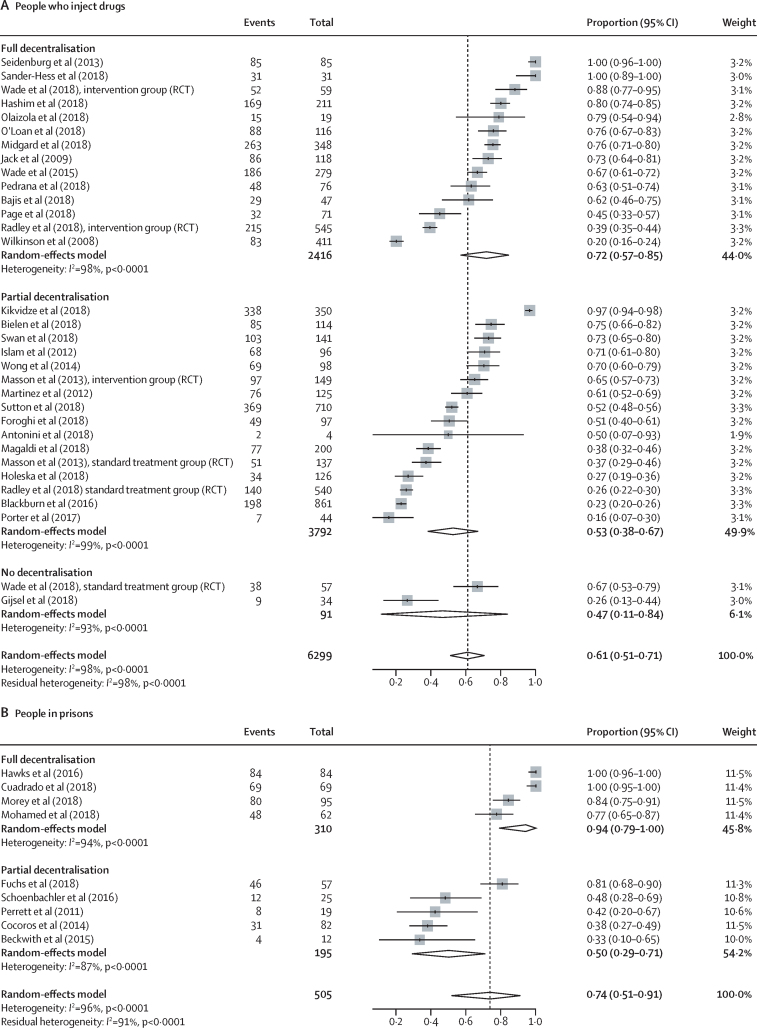
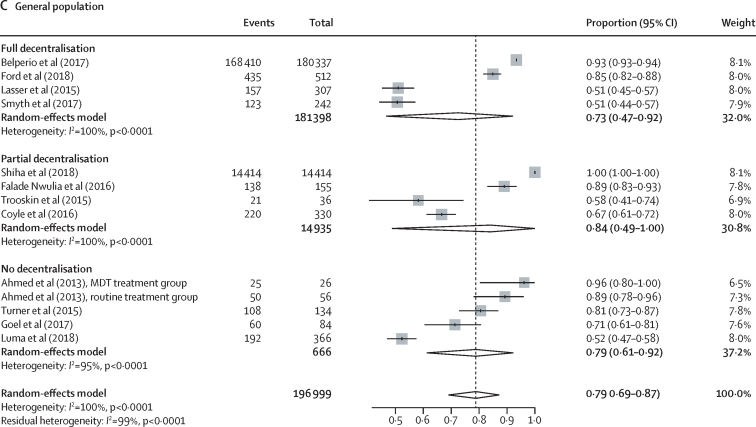
Findings: Our search identified 8050 reports, of which 132 met the eligibility criteria, and an additional ten reports were identified from reference citations and grey literature. Therefore, the final synthesis included 142 studies from 34 countries (20 [14%] studies from low-income and middle-income countries) and a total of 489 996 patients (239 446 [49%] from low-income and middle-income countries). Rates of linkage to care were higher with full decentralisation compared with partial or no decentralisation among people who inject drugs (full 72% [95% CI 57-85] vs partial 53% [38-67] vs none 47% [11-84]) and among people in prisons (full 94% [79-100] vs partial 50% [29-71]), although the CIs overlap for people who inject drugs. Similarly, treatment uptake was higher with full decentralisation compared with partial or no decentralisation (people who inject drugs: full 73% [65-80] vs partial 66% [55-77] vs none 35% [23-48]; people in prisons: full 72% [48-91] vs partial 39% [17-63]), although CIs overlap for full versus partial decentralisation. The results in the general population studies were more heterogeneous. SVR12 rates were high (≥90%) across different levels of decentralisation in all populations. Task-shifting of care and treatment to a non-specialist was associated with similar SVR12 rates to treatment delivered by specialists. There was a severe or critical risk of bias for 46% of studies, and heterogeneity across studies tended to be very high (I2>90%).
Interpretation: Decentralisation and integration of HCV care to harm-reduction sites or primary care showed some evidence of improved access to testing, linkage to care, and treatment, and task-shifting of care and treatment to non-specialists was associated with similarly high cure rates to care delivered by specialists, across a range of populations and settings. These findings provide support for the adoption of decentralisation and task-shifting to non-specialists in national HCV programmes.
Funding: Unitaid.
© 2021 World Health Organization; licensee Elsevier. This is an Open Access article published under the CC BY 3.0 IGO license which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. In any use of this article, there should be no suggestion that WHO endorses any specific organisation, products or services. The use of the WHO logo is not permitted. This notice should be preserved along with the article's original URL.
Figures
Comment in
-
Decentralisation, integration, and task-shifting: tools to accelerate the elimination of hepatitis C.Lancet Glob Health. 2021 Apr;9(4):e375-e376. doi: 10.1016/S2214-109X(21)00055-3. Epub 2021 Feb 24. Lancet Glob Health. 2021. PMID: 33639098 No abstract available.
References
-
- WHO Global hepatitis report, 2017. April, 2017. https://www.who.int/hepatitis/publications/global-hepatitis-report2017/en
-
- WHO Global health sector strategy on viral hepatitis 2016–2021. June, 2016. http://www.who.int/hepatitis/strategy2016-2021/ghss-hep/en
-
- WHO Global report on access to hepatitis C treatment: focus on overcoming barriers. October, 2016. https://apps.who.int/iris/handle/10665/250625
-
- WHO Progress report on HIV, viral hepatitis and sexually transmitted infections 2019. July, 2019. https://www.who.int/hiv/strategy2016-2021/progress-report-2019/en
-
- Easterbrook PJ, WHO Guidelines Development Group Who to test and how to test for chronic hepatitis C infection—2016 WHO testing guidance for low- and middle-income countries. J Hepatol. 2016;65(suppl):S46–S66. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
