

Levothyroxine and the risk of adverse pregnancy outcomes in women with subclinical hypothyroidism: a systematic review and meta-analysis
- PMID: 33639909
- PMCID: PMC7912520
- DOI: 10.1186/s12902-021-00699-5
Levothyroxine and the risk of adverse pregnancy outcomes in women with subclinical hypothyroidism: a systematic review and meta-analysis
Abstract
Background: Levothyroxine replacement therapy may decrease the risk of adverse pregnancy outcomes among women with subclinical hypothyroidism (SCH). The aim of this study is to conduct a systematic review and meta-analysis to examine the risk of adverse pregnancy, perinatal, and early childhood outcomes among women with SCH treated with levothyroxine.
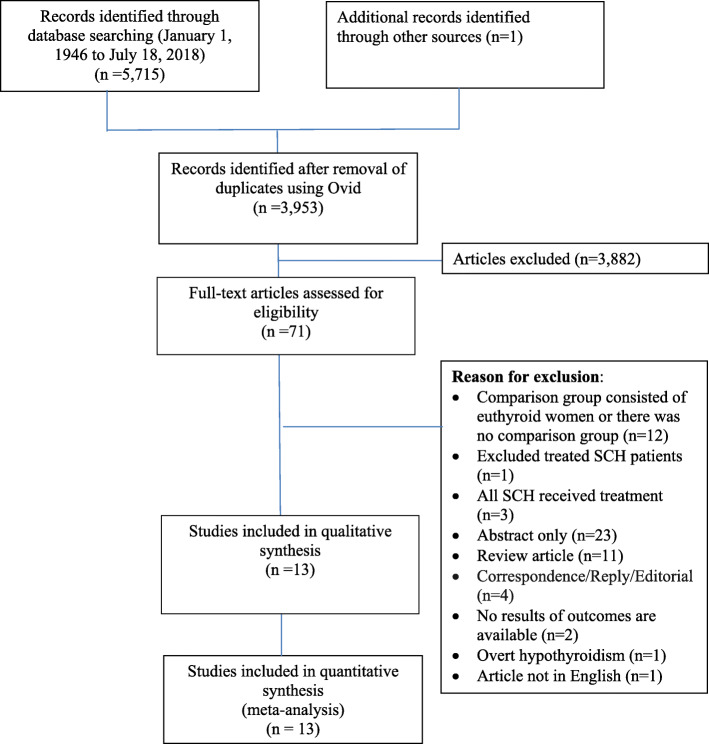
Methods: A systematic literature search was conducted using Ovid-Medline, Ovid-EMBASE, Pubmed (non-Medline), Ebsco-CINAHL Plus with full text and Cochrane Library databases. Randomized controlled studies (RCTs) and observational studies examining the association between treatment of SCH during pregnancy and our outcomes of interest were included. Studies that compared levothyroxine treatment versus no treatment were eligible for inclusion. Data from included studies were extracted and quality assessment was performed by two independent reviewers.
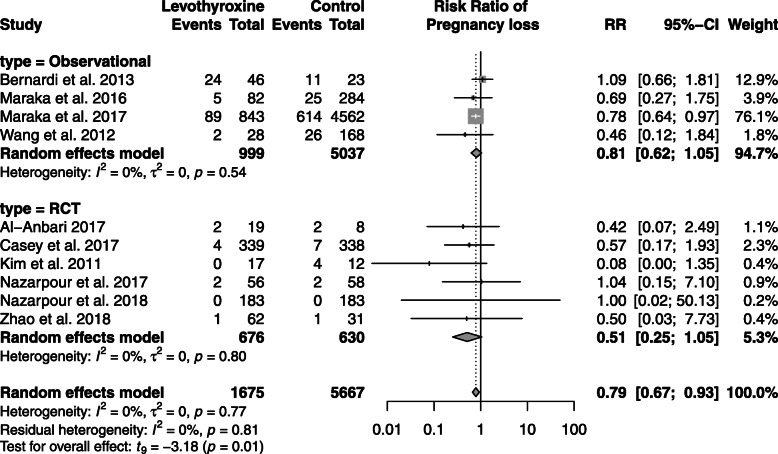
Results: Seven RCTs and six observational studies met our inclusion criteria. A total of 7342 individuals were included in these studies. RCTs demonstrated several sources of bias, with lack of blinding of the participants or research personnel; only one study was fully blinded. In the observational studies, there was moderate to serious risk of bias due to lack of adjustment for certain confounding variables, participant selection, and selective reporting of results. Pooled analyses showed decreased risk of pregnancy loss (RR: 0.79; 95% CI: 0.67 to 0.93) and neonatal death (RR: 0.35; 95% CI: 0.17 to 0.72) associated with levothyroxine treatment during pregnancy among women with SCH. There were no associations between levothyroxine treatment and outcomes during labour and delivery, or cognitive status in children at 3 or 5 years of age.
Conclusion: Treatment of SCH with levothyroxine during pregnancy is associated with decreased risks of pregnancy loss and neonatal death. Given the paucity of available data and heterogeneity of included studies, additional studies are needed to address the benefits of levothyroxine use among pregnant women with SCH.
Keywords: Levothyroxine; Pregnancy outcomes; Subclinical hypothyroidism.
Conflict of interest statement
No conflict of interests to declare.
Figures

References
-
- Negro R, Stagnaro-Green A. Diagnosis and management of subclinical hypothyroidism in pregnancy. BMJ (Clinical research ed) 2014;349:g4929. - PubMed
-
- van den Boogaard E, Vissenberg R, Land JA, van Wely M, van der Post JA, Goddijn M, Bisschop PH. Significance of (sub) clinical thyroid dysfunction and thyroid autoimmunity before conception and in early pregnancy: a systematic review. Hum Reprod Update. 2011;17(5):605–619. doi: 10.1093/humupd/dmr024. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
