

Clinical experience with the AKT1 inhibitor miransertib in two children with PIK3CA-related overgrowth syndrome
- PMID: 33639990
- PMCID: PMC7913425
- DOI: 10.1186/s13023-021-01745-0
Clinical experience with the AKT1 inhibitor miransertib in two children with PIK3CA-related overgrowth syndrome
Abstract
Background: PIK3CA-related overgrowth spectrum (PROS) refers to a group of rare disorders, caused by somatic activating mutations in PIK3CA, resulting in abnormal PI3K-AKT-mTOR pathway signalling. Significant associated morbidity is frequently observed, and approved treatments are lacking. Miransertib (ARQ 092) is a novel, orally available, selective pan-AKT inhibitor with proven in vitro efficacy. Following recent results of the use of AKT inhibitors in Proteus syndrome (PS) and AKT-mutant cancers, we investigated its therapeutic use in two patients with severe PROS who had exhausted conventional treatment methods.
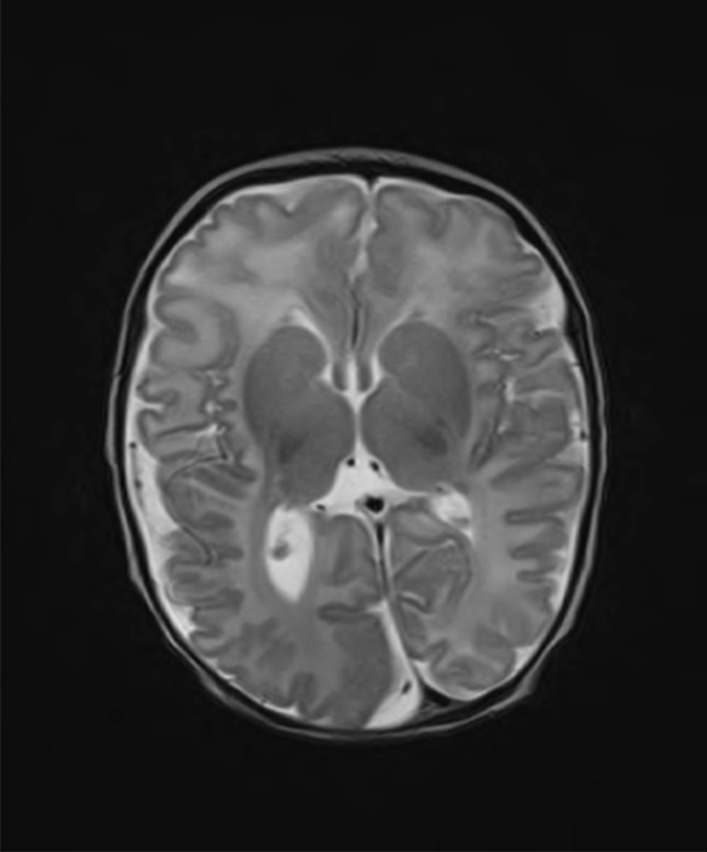
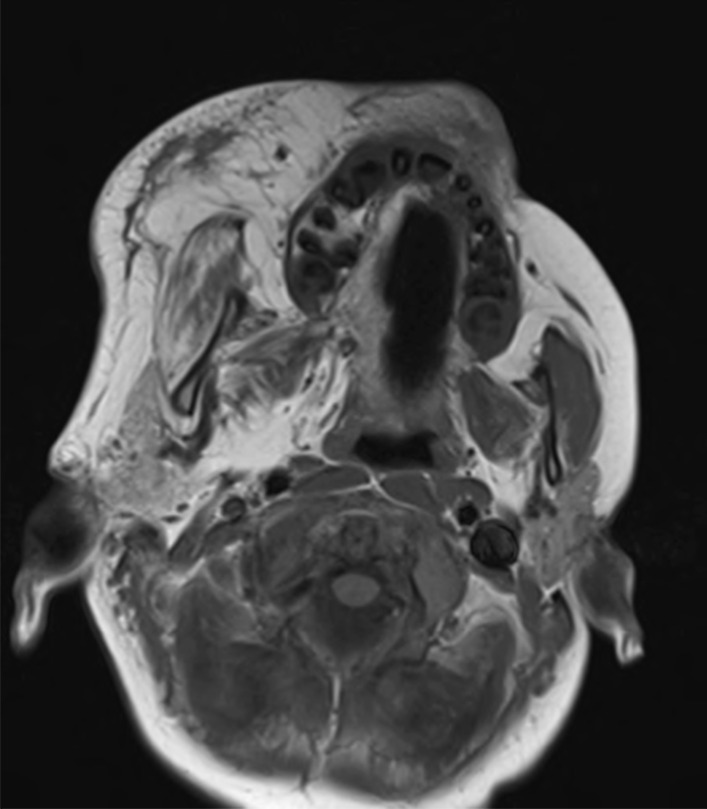
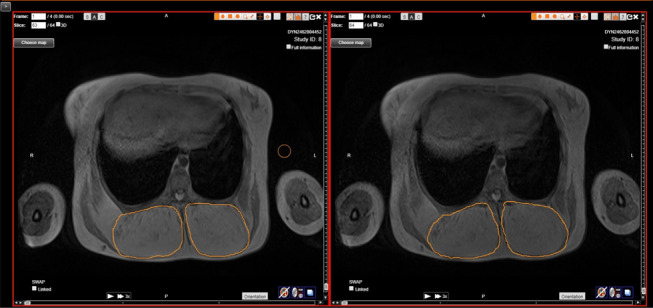
Results: Two patients, one with CLOVES variant (P1) and one with facial infiltrating lipomatosis and hemimegalencephaly (P2), were commenced on miransertib treatment on a compassionate use basis. In patient one, intra-abdominal and paraspinal overgrowth had resulted in respiratory compromise, obstructive uropathy, dysfunctional seating and lying postures, and chronic pain. In patient two, hemifacial overgrowth and hemimegalencephaly had caused difficulties with articulation and oral function, and refractory epilepsy. Miransertib treatment was continued for a median duration of 22 months (range 22-28). In patient one, alleviation of respiratory compromise was observed and functionally, seating and lying postures improved. Serial volumetric MRI analysis revealed 15% reduction in calculated volumes of fatty overgrowth between treatment commencement and end. In patient two, reduction in seizure burden and improved parent-reported quality of life measures were reported. Treatment was discontinued in both patients due to lack of sustained response, and poor compliance in year two of treatment (P2). No significant toxicities were reported.
Conclusion: We report the first paediatric case series of the use of miransertib in two children with PROS. Objective clinical response was observed in patient one, and improvement in key qualitative outcomes was reported in patient two. Treatment was well tolerated with no significant toxicities reported. This case series highlights the potential therapeutic utility of miransertib in selected paediatric patients with severe PROS, and further demonstrates the potential for re-purposing targeted therapies for the treatment of rare diseases. An open label, Phase 1/2 study of miransertib in children with PROS and PS is underway to more accurately assess the efficacy of miransertib in the treatment of PROS disorder (NCT03094832).
Keywords: AKT inhibitor; Miransertib; Next generation sequencing (NGS); PIK3CA-related overgrowth spectrum (PROS); Targeted treatment.
Conflict of interest statement
Miransertib was provided by ArQule Inc. (Burlington MA) on a compassionate managed patient access programme basis for the duration of the study period.
Figures
References
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
