

Risk predictors of progression to severe disease during the febrile phase of dengue: a systematic review and meta-analysis
- PMID: 33640077
- PMCID: PMC8240557
- DOI: 10.1016/S1473-3099(20)30601-0
Risk predictors of progression to severe disease during the febrile phase of dengue: a systematic review and meta-analysis
Abstract
Background: The ability to accurately predict early progression of dengue to severe disease is crucial for patient triage and clinical management. Previous systematic reviews and meta-analyses have found significant heterogeneity in predictors of severe disease due to large variation in these factors during the time course of the illness. We aimed to identify factors associated with progression to severe dengue disease that are detectable specifically in the febrile phase.
Methods: We did a systematic review and meta-analysis to identify predictors identifiable during the febrile phase associated with progression to severe disease defined according to WHO criteria. Eight medical databases were searched for studies published from Jan 1, 1997, to Jan 31, 2020. Original clinical studies in English assessing the association of factors detected during the febrile phase with progression to severe dengue were selected and assessed by three reviewers, with discrepancies resolved by consensus. Meta-analyses were done using random-effects models to estimate pooled effect sizes. Only predictors reported in at least four studies were included in the meta-analyses. Heterogeneity was assessed using the Cochrane Q and I2 statistics, and publication bias was assessed by Egger's test. We did subgroup analyses of studies with children and adults. The study is registered with PROSPERO, CRD42018093363.
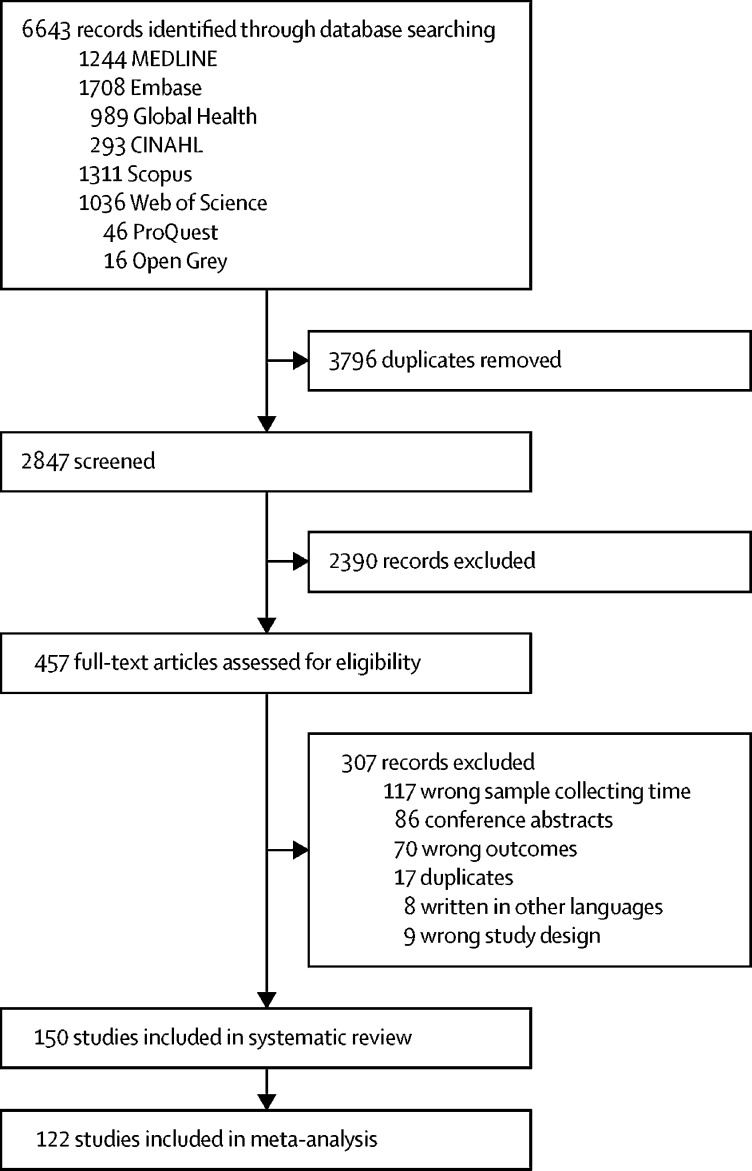
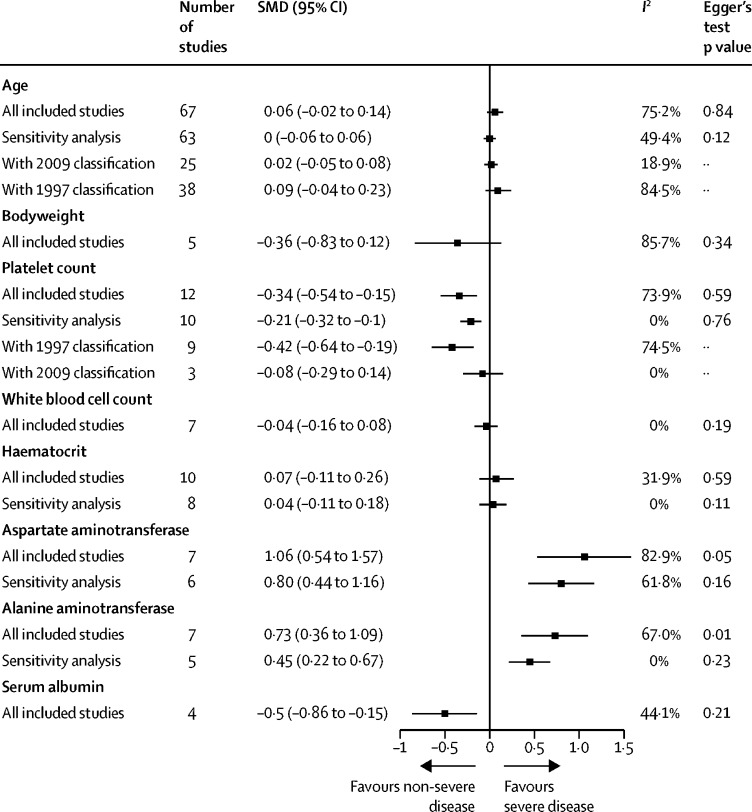
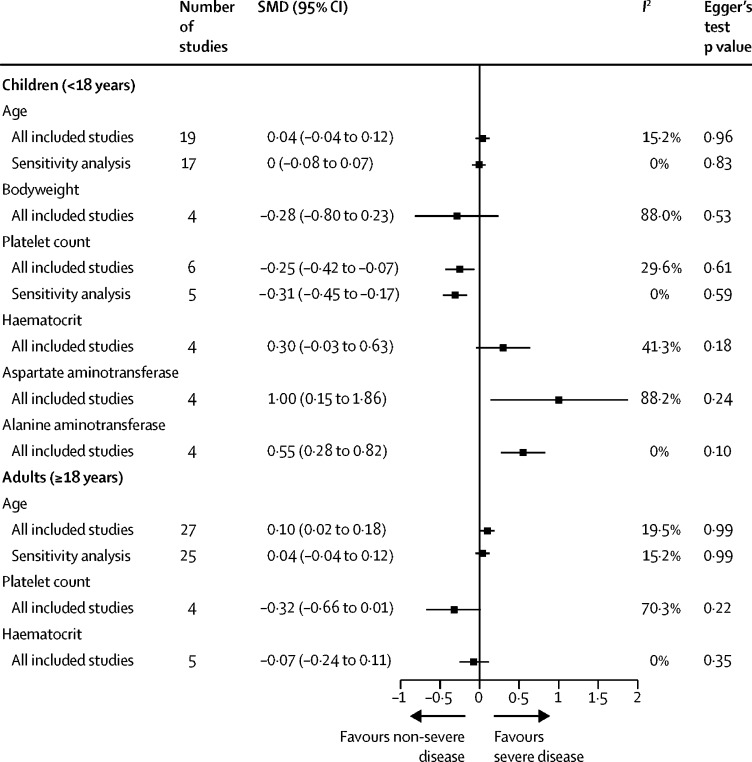
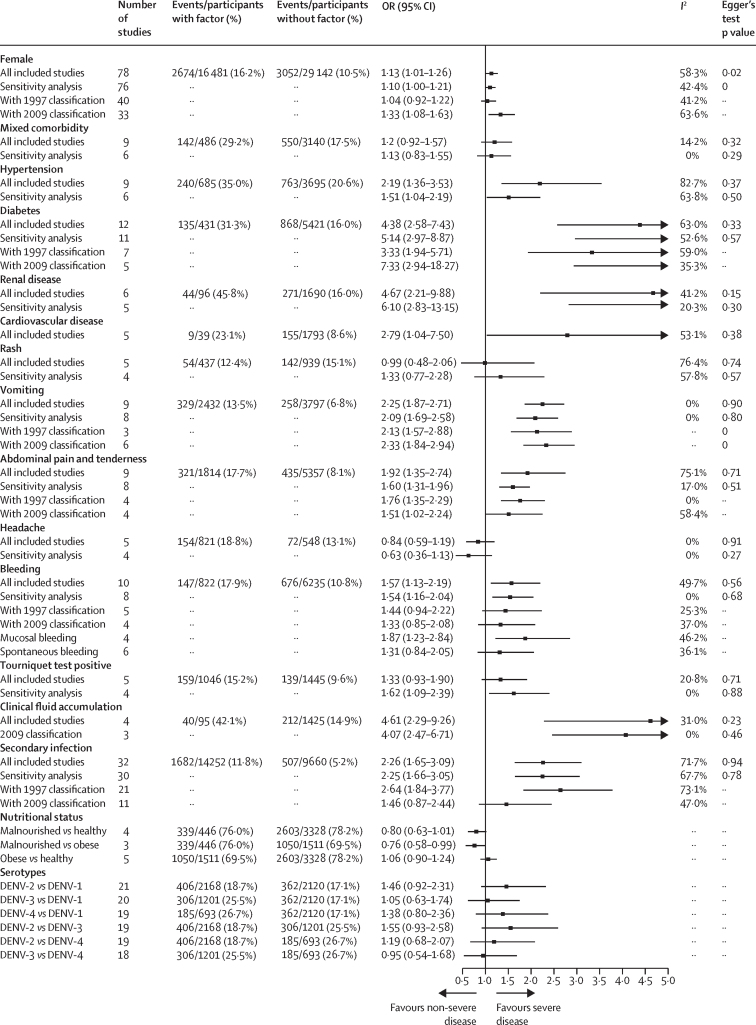
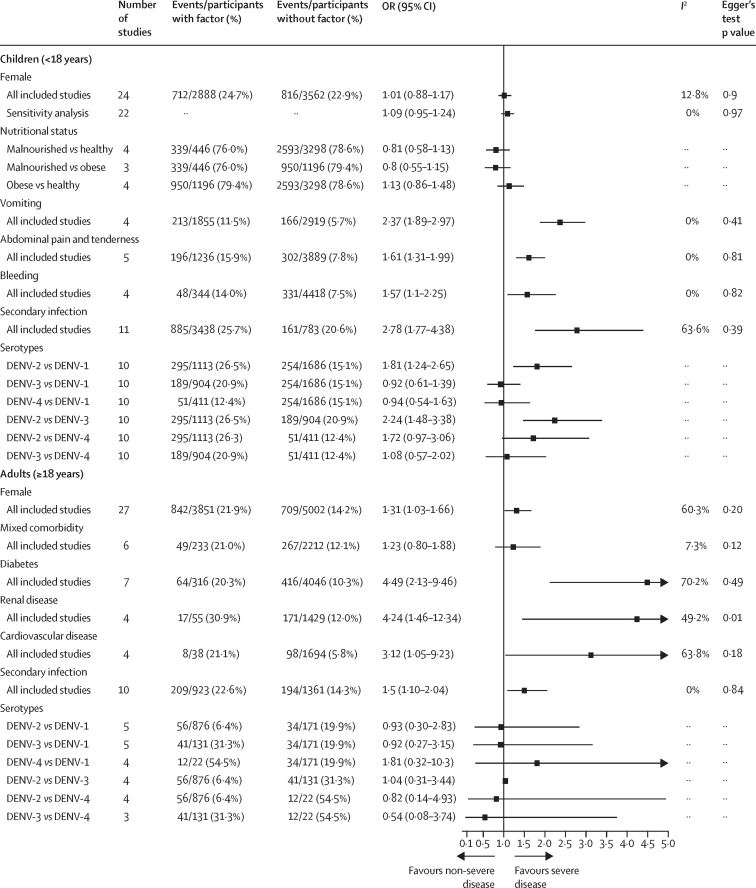
Findings: Of 6643 studies identified, 150 articles were included in the systematic review, and 122 articles comprising 25 potential predictors were included in the meta-analyses. Female patients had a higher risk of severe dengue than male patients in the main analysis (2674 [16·2%] of 16 481 vs 3052 [10·5%] of 29 142; odds ratio [OR] 1·13 [95% CI 1·01-1·26) but not in the subgroup analysis of studies with children. Pre-existing comorbidities associated with severe disease were diabetes (135 [31·3%] of 431 with vs 868 [16·0%] of 5421 without; crude OR 4·38 [2·58-7·43]), hypertension (240 [35·0%] of 685 vs 763 [20·6%] of 3695; 2·19 [1·36-3·53]), renal disease (44 [45·8%] of 96 vs 271 [16·0%] of 1690; 4·67 [2·21-9·88]), and cardiovascular disease (nine [23·1%] of 39 vs 155 [8·6%] of 1793; 2·79 [1·04-7·50]). Clinical features during the febrile phase associated with progression to severe disease were vomiting (329 [13·5%] of 2432 with vs 258 [6·8%] of 3797 without; 2·25 [1·87-2·71]), abdominal pain and tenderness (321 [17·7%] of 1814 vs 435 [8·1%] of 5357; 1·92 [1·35-2·74]), spontaneous or mucosal bleeding (147 [17·9%] of 822 vs 676 [10·8%] of 6235; 1·57 [1·13-2·19]), and the presence of clinical fluid accumulation (40 [42·1%] of 95 vs 212 [14·9%] of 1425; 4·61 [2·29-9·26]). During the first 4 days of illness, platelet count was lower (standardised mean difference -0·34 [95% CI -0·54 to -0·15]), serum albumin was lower (-0·5 [-0·86 to -0·15]), and aminotransferase concentrations were higher (aspartate aminotransferase [AST] 1·06 [0·54 to 1·57] and alanine aminotransferase [ALT] 0·73 [0·36 to 1·09]) among individuals who progressed to severe disease. Dengue virus serotype 2 was associated with severe disease in children. Secondary infections (vs primary infections) were also associated with severe disease (1682 [11·8%] of 14 252 with vs 507 [5·2%] of 9660 without; OR 2·26 [95% CI 1·65-3·09]). Although the included studies had a moderate to high risk of bias in terms of study confounding, the risk of bias was low to moderate in other domains. Heterogeneity of the pooled results varied from low to high on different factors.
Interpretation: This analysis supports monitoring of the warning signs described in the 2009 WHO guidelines on dengue. In addition, testing for infecting serotype and monitoring platelet count and serum albumin, AST, and ALT concentrations during the febrile phase of illness could improve the early prediction of severe dengue.
Funding: Wellcome Trust, National Institute for Health Research, Collaborative Project to Increase Production of Rural Doctors, and Royal Thai Government.
Copyright © 2021 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Figures
Comment in
-
Transaminases and serum albumin as early predictors of severe dengue.Lancet Infect Dis. 2021 Nov;21(11):1488-1489. doi: 10.1016/S1473-3099(21)00583-1. Lancet Infect Dis. 2021. PMID: 34717802 No abstract available.
-
Transaminases and serum albumin as early predictors of severe dengue - Authors' reply.Lancet Infect Dis. 2021 Nov;21(11):1489-1490. doi: 10.1016/S1473-3099(21)00624-1. Lancet Infect Dis. 2021. PMID: 34717803 No abstract available.
References
-
- Schaffner F, Mathis A. Dengue and dengue vectors in the WHO European region: past, present, and scenarios for the future. Lancet Infect Dis. 2014;14:1271–1280. - PubMed
-
- WHO . new edition. World Health Organization; Geneva: 2009. Dengue guidelines for diagnosis, treatment, prevention and control. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
