

Increased apolipoprotein-B:A1 ratio predicts cardiometabolic risk in patients with juvenile onset SLE
- PMID: 33640328
- PMCID: PMC7992074
- DOI: 10.1016/j.ebiom.2021.103243
Increased apolipoprotein-B:A1 ratio predicts cardiometabolic risk in patients with juvenile onset SLE
Abstract
Background: Cardiovascular disease is a leading cause of mortality in patients with juvenile-onset systemic lupus erythematosus (JSLE). Traditional factors for cardiovascular risk (CVR) prediction are less robust in younger patients. More reliable CVR biomarkers are needed for JSLE patient stratification and to identify therapeutic approaches to reduce cardiovascular morbidity and mortality in JSLE.
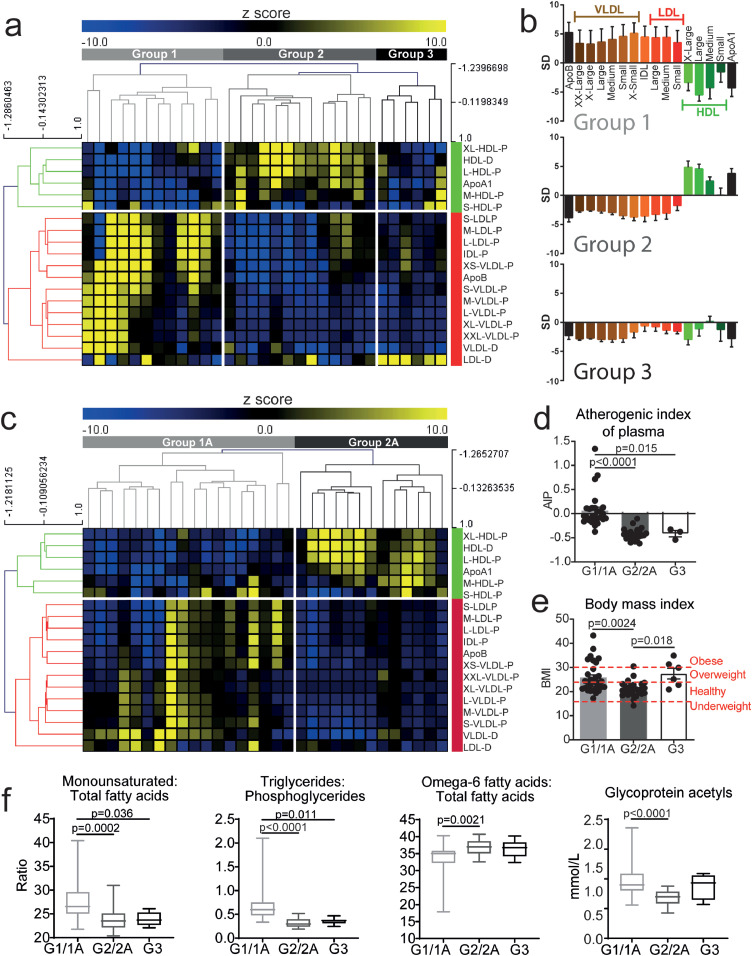
Methods: Serum metabolomic analysis (including >200 lipoprotein measures) was performed on a discovery (n=31, median age 19) and validation (n=31, median age 19) cohort of JSLE patients. Data was analysed using cluster, receiver operating characteristic analysis and logistic regression. RNA-sequencing assessed gene expression in matched patient samples.
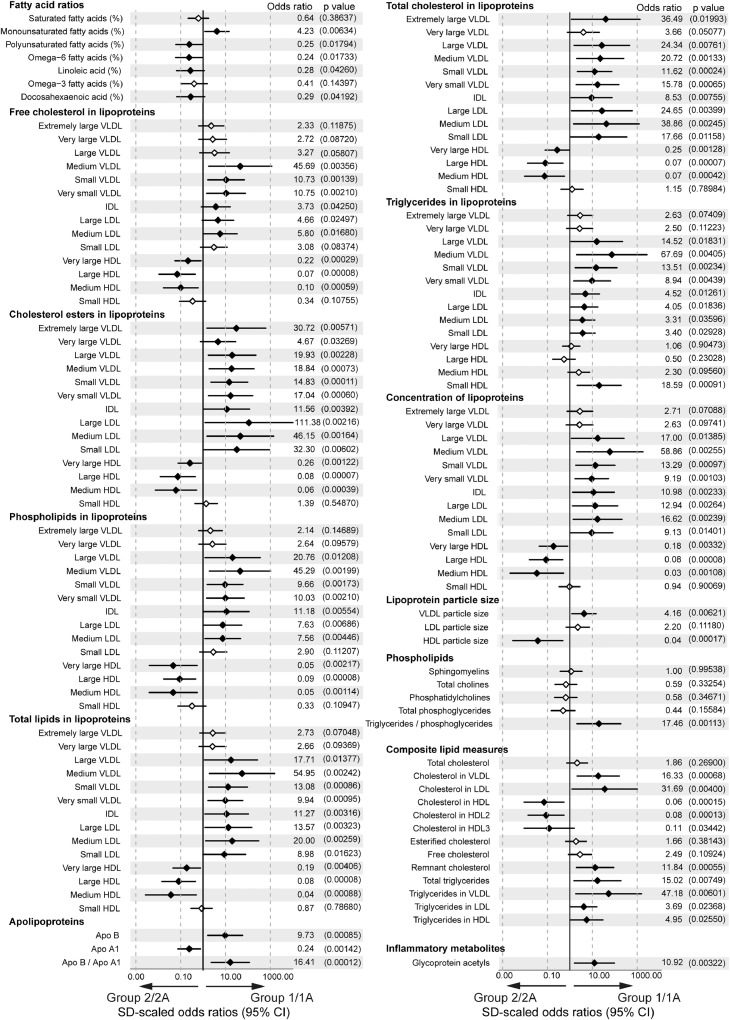
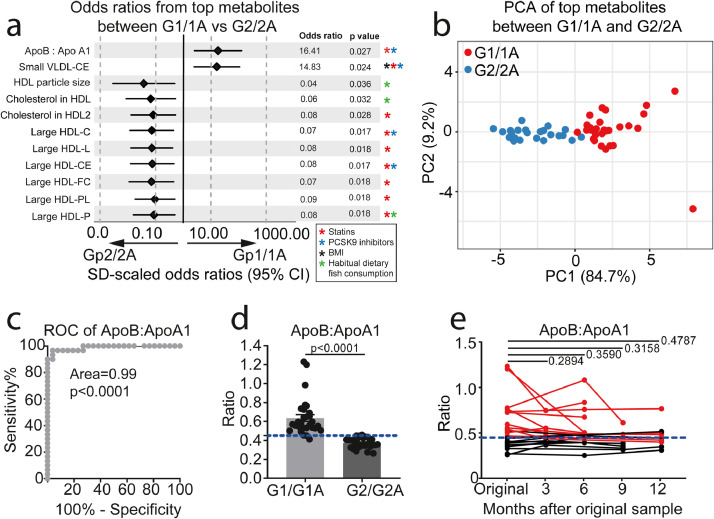
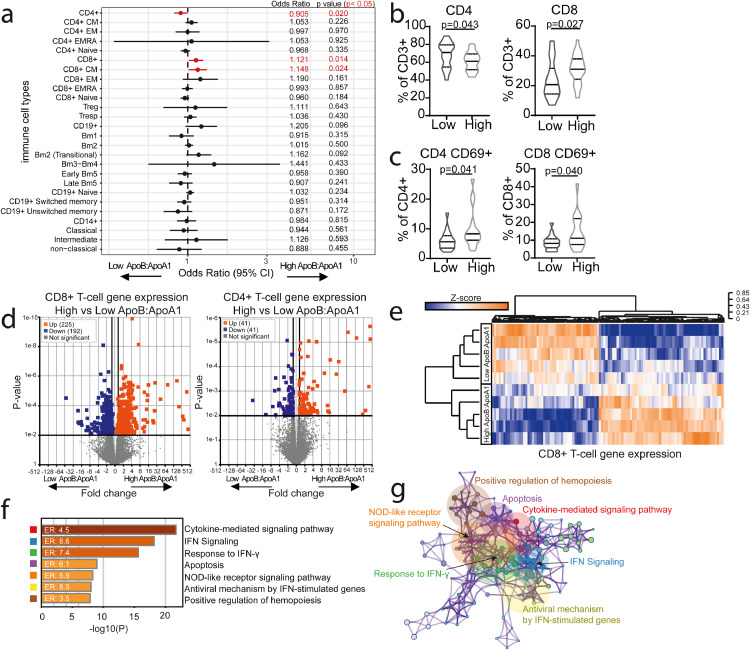
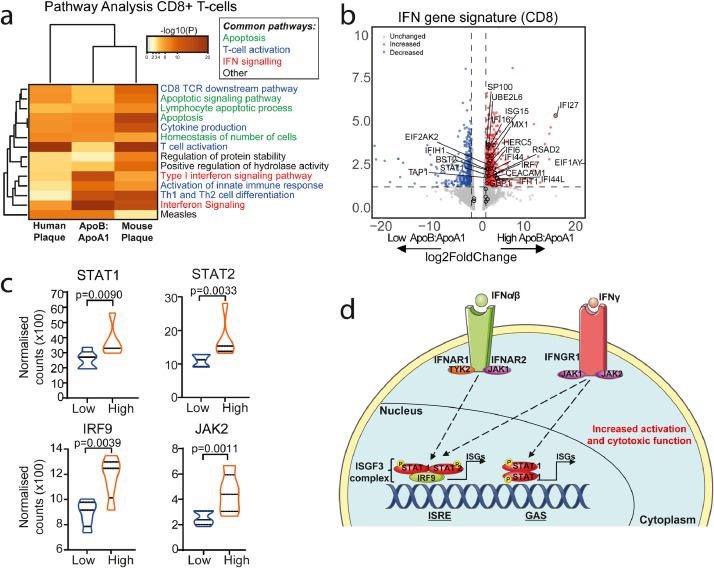
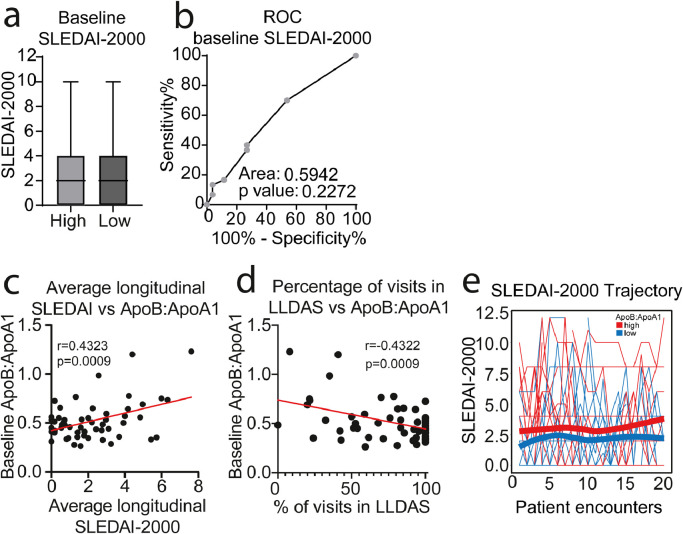
Findings: Hierarchical clustering of lipoprotein measures identified and validated two unique JSLE groups. Group-1 had an atherogenic and Group-2 had an atheroprotective lipoprotien profile. Apolipoprotein(Apo)B:ApoA1 distinguished the two groups with high specificity (96.2%) and sensitivity (96.7%). JSLE patients with high ApoB:ApoA1 ratio had increased CD8+ T-cell frequencies and a CD8+ T-cell transcriptomic profile enriched in genes associated with atherogenic processes including interferon signaling. These metabolic and immune signatures overlapped statistically significantly with lipid biomarkers associated with sub-clinical atherosclerosis in adult SLE patients and with genes overexpressed in T-cells from human atherosclerotic plaque respectively. Finally, baseline ApoB:ApoA1 ratio correlated positively with SLE disease activity index (r=0.43, p=0.0009) and negatively with Lupus Low Disease Activity State (r=-0.43, p=0.0009) over 5-year follow-up.
Interpretation: Multi-omic analysis identified high ApoB:ApoA1 as a potential biomarker of increased cardiometabolic risk and worse clinical outcomes in JSLE. ApoB:ApoA1 could help identify patients that require increased disease monitoring, lipid modification or lifestyle changes.
Funding: Lupus UK, The Rosetrees Trust, British Heart Foundation, UCL & Birkbeck MRC Doctoral Training Programme and Versus Arthritis.
Keywords: CD8+ T cells; Cardiovascular disease; Interferon; Juvenile-onset systemic lupus erythematosus; Lipids.
Copyright © 2021 The Author(s). Published by Elsevier B.V. All rights reserved.
Conflict of interest statement
Declaration of Competing Interest The authors have declared that no conflict of interest exists.
Figures
Comment in
-
How to predict the prognosis in juvenile-onset SLE?EBioMedicine. 2021 Apr;66:103285. doi: 10.1016/j.ebiom.2021.103285. Epub 2021 Mar 25. EBioMedicine. 2021. PMID: 33774330 Free PMC article. No abstract available.
Similar articles
-
Clinical and laboratory characteristics in juvenile-onset systemic lupus erythematosus across age groups.Lupus. 2020 Apr;29(5):474-481. doi: 10.1177/0961203320909156. Epub 2020 Mar 31. Lupus. 2020. PMID: 32233733 Free PMC article.
-
Systemic lupus erythematosus patients have unique changes in serum metabolic profiles across age associated with cardiometabolic risk.Rheumatology (Oxford). 2024 Oct 1;63(10):2741-2753. doi: 10.1093/rheumatology/kead646. Rheumatology (Oxford). 2024. PMID: 38048621 Free PMC article.
-
Pitavastatin: novel effects on lipid parameters.Atheroscler Suppl. 2011 Nov;12(3):277-84. doi: 10.1016/S1567-5688(11)70887-X. Atheroscler Suppl. 2011. PMID: 22152282 Review.
-
The diagnostic value of the combined application of blood lipid metabolism markers and interleukin-6 in osteoporosis and osteopenia.Lipids Health Dis. 2025 Feb 5;24(1):38. doi: 10.1186/s12944-025-02456-2. Lipids Health Dis. 2025. PMID: 39910539 Free PMC article.
-
Dietary, macronutrient, micronutrient, and nutrigenetic factors impacting cardiovascular risk markers apolipoprotein B and apolipoprotein A1: a narrative review.Nutr Rev. 2024 Jun 10;82(7):949-962. doi: 10.1093/nutrit/nuad102. Nutr Rev. 2024. PMID: 37615981 Review.
Cited by
-
Metabolomics in juvenile idiopathic arthritis: A distinct profile in patients under methotrexate.Clinics (Sao Paulo). 2025 Jan 28;80:100522. doi: 10.1016/j.clinsp.2024.100522. eCollection 2025. Clinics (Sao Paulo). 2025. PMID: 39879909 Free PMC article.
-
Impact of puberty, sex determinants and chronic inflammation on cardiovascular risk in young people.Front Cardiovasc Med. 2023 Jun 27;10:1191119. doi: 10.3389/fcvm.2023.1191119. eCollection 2023. Front Cardiovasc Med. 2023. PMID: 37441710 Free PMC article. Review.
-
Lipid Metabolism: Immune Regulation and Therapeutic Prospectives in Systemic Lupus Erythematosus.Front Immunol. 2022 Mar 18;13:860586. doi: 10.3389/fimmu.2022.860586. eCollection 2022. Front Immunol. 2022. PMID: 35371016 Free PMC article. Review.
-
Gut microbiota landscape and potential biomarker identification in female patients with systemic lupus erythematosus using machine learning.Front Cell Infect Microbiol. 2023 Dec 19;13:1289124. doi: 10.3389/fcimb.2023.1289124. eCollection 2023. Front Cell Infect Microbiol. 2023. PMID: 38169617 Free PMC article.
-
Serum apolipoprotein B to apolipoprotein A-I ratio predicts mortality in patients with heart failure.ESC Heart Fail. 2024 Feb;11(1):99-111. doi: 10.1002/ehf2.14547. Epub 2023 Oct 11. ESC Heart Fail. 2024. PMID: 37822135 Free PMC article.
References
-
- Bernatsky S, Boivin J-F, Joseph L, Manzi S, Ginzler E, Gladman DD. Mortality in systemic lupus erythematosus. Arthritis Rheumatism. 2006;54(8):2550–2557. - PubMed
-
- Nossent J, Cikes N, Kiss E, Marchesoni A, Nassonova V, Mosca M. Current causes of death in systemic lupus erythematosus in Europe, 2000—2004: relation to disease activity and damage accrual. Lupus. 2007;16(5):309–317. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
