

Normal Tissue Injury Induced by Photon and Proton Therapies: Gaps and Opportunities
- PMID: 33640423
- PMCID: PMC8496269
- DOI: 10.1016/j.ijrobp.2021.02.043
Normal Tissue Injury Induced by Photon and Proton Therapies: Gaps and Opportunities
Abstract
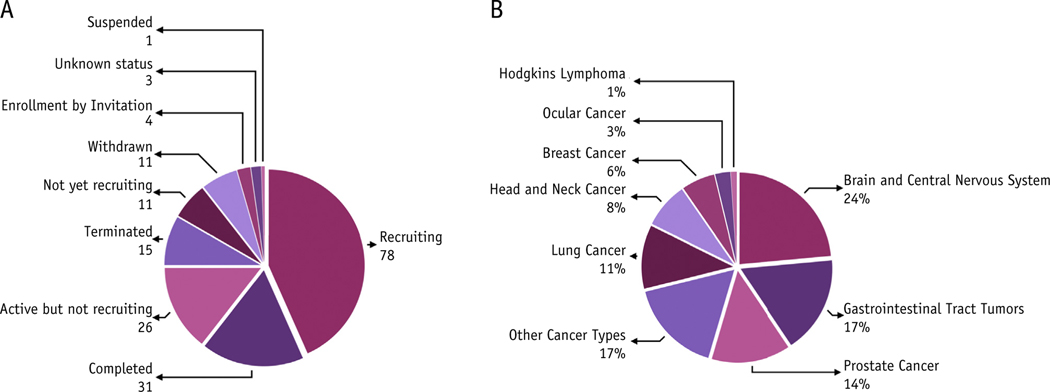
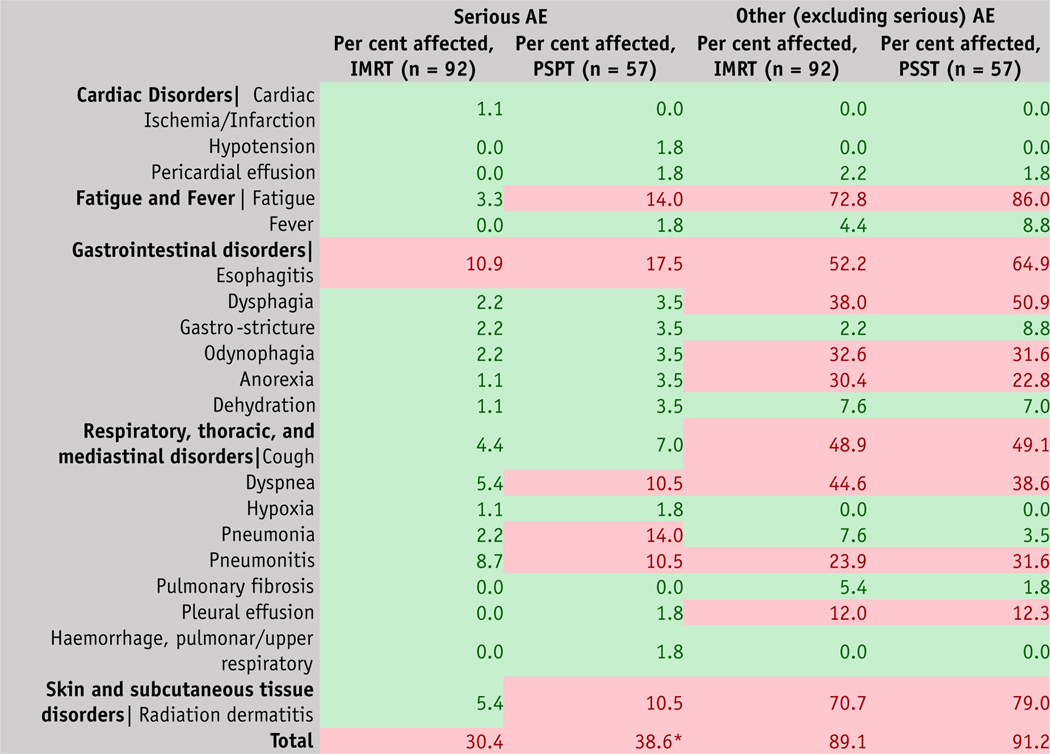
Despite technological advances in radiation therapy (RT) and cancer treatment, patients still experience adverse effects. Proton therapy (PT) has emerged as a valuable RT modality that can improve treatment outcomes. Normal tissue injury is an important determinant of the outcome; therefore, for this review, we analyzed 2 databases: (1) clinical trials registered with ClinicalTrials.gov and (2) the literature on PT in PubMed, which shows a steady increase in the number of publications. Most studies in PT registered with ClinicalTrials.gov with results available are nonrandomized early phase studies with a relatively small number of patients enrolled. From the larger database of nonrandomized trials, we listed adverse events in specific organs/sites among patients with cancer who are treated with photons and protons to identify critical issues. The present data demonstrate dosimetric advantages of PT with favorable toxicity profiles and form the basis for comparative randomized prospective trials. A comparative analysis of 3 recently completed randomized trials for normal tissue toxicities suggests that for early stage non-small cell lung cancer, no meaningful comparison could be made between stereotactic body RT and stereotactic body PT due to low accrual (NCT01511081). In addition, for locally advanced non-small cell lung cancer, a comparison of intensity modulated RT with passive scattering PT (now largely replaced by spot-scanned intensity modulated PT), PT did not provide any benefit in normal tissue toxicity or locoregional failure over photon therapy. Finally, for locally advanced esophageal cancer, proton beam therapy provided a lower total toxicity burden but did not improve progression-free survival and quality of life (NCT01512589). The purpose of this review is to inform the limitations of current trials looking at protons and photons, considering that advances in technology, physics, and biology are a continuum, and to advocate for future trials geared toward accurate precision RT that need to be viewed as an iterative process in a defined path toward delivering optimal radiation treatment. A foundational understanding of the radiobiologic differences between protons and photons in tumor and normal tissue responses is fundamental to, and necessary for, determining the suitability of a given type of biologically optimized RT to a patient or cohort.
Published by Elsevier Inc.
Figures
Similar articles
-
Establishing Evidence-Based Indications for Proton Therapy: An Overview of Current Clinical Trials.Int J Radiat Oncol Biol Phys. 2017 Feb 1;97(2):228-235. doi: 10.1016/j.ijrobp.2016.10.045. Epub 2016 Nov 8. Int J Radiat Oncol Biol Phys. 2017. PMID: 28068231
-
Initial Report of a Prospective Dosimetric and Clinical Feasibility Trial Demonstrates the Potential of Protons to Increase the Therapeutic Ratio in Breast Cancer Compared With Photons.Int J Radiat Oncol Biol Phys. 2016 May 1;95(1):411-421. doi: 10.1016/j.ijrobp.2015.09.018. Epub 2015 Sep 25. Int J Radiat Oncol Biol Phys. 2016. PMID: 26611875
-
Spatial Dose Patterns Associated With Radiation Pneumonitis in a Randomized Trial Comparing Intensity-Modulated Photon Therapy With Passive Scattering Proton Therapy for Locally Advanced Non-Small Cell Lung Cancer.Int J Radiat Oncol Biol Phys. 2019 Aug 1;104(5):1124-1132. doi: 10.1016/j.ijrobp.2019.02.039. Epub 2019 Feb 26. Int J Radiat Oncol Biol Phys. 2019. PMID: 30822531 Clinical Trial.
-
Proton therapy for locally advanced non-small cell lung cancer.Br J Radiol. 2020 Mar;93(1107):20190378. doi: 10.1259/bjr.20190378. Epub 2019 Aug 20. Br J Radiol. 2020. PMID: 31430188 Free PMC article. Review.
-
Consensus Statement on Proton Therapy in Early-Stage and Locally Advanced Non-Small Cell Lung Cancer.Int J Radiat Oncol Biol Phys. 2016 May 1;95(1):505-516. doi: 10.1016/j.ijrobp.2016.01.036. Epub 2016 Jan 23. Int J Radiat Oncol Biol Phys. 2016. PMID: 27084663 Free PMC article. Review.
Cited by
-
Radiation induced lung injury (RILI) after postoperative intensity modulated proton therapy (IMPT) in a patient with stage III locally advanced lung adenocarcinoma: a case report.Transl Cancer Res. 2022 Sep;11(9):3400-3408. doi: 10.21037/tcr-22-256. Transl Cancer Res. 2022. PMID: 36237266 Free PMC article.
-
Metabolic response to radiation therapy in cancer.Mol Carcinog. 2022 Feb;61(2):200-224. doi: 10.1002/mc.23379. Epub 2021 Dec 27. Mol Carcinog. 2022. PMID: 34961986 Free PMC article. Review.
-
Addressing challenges in low-income and middle-income countries through novel radiotherapy research opportunities.Lancet Oncol. 2024 Jun;25(6):e270-e280. doi: 10.1016/S1470-2045(24)00038-X. Lancet Oncol. 2024. PMID: 38821101 Free PMC article. Review.
-
Mechanisms and Review of Clinical Evidence of Variations in Relative Biological Effectiveness in Proton Therapy.Int J Radiat Oncol Biol Phys. 2022 Jan 1;112(1):222-236. doi: 10.1016/j.ijrobp.2021.08.015. Epub 2021 Aug 15. Int J Radiat Oncol Biol Phys. 2022. PMID: 34407443 Free PMC article. Review.
-
CD9- and CD81-positive extracellular vesicles provide a marker to monitor glioblastoma cell response to photon-based and proton-based radiotherapy.Front Oncol. 2022 Sep 20;12:947439. doi: 10.3389/fonc.2022.947439. eCollection 2022. Front Oncol. 2022. PMID: 36203458 Free PMC article.
References
-
- Atun R, Jaffray DA, Barton MB, et al. Expanding global access to radiotherapy. Lancet Oncol 2015;16:1153–1186. - PubMed
-
- Thariat J, Hannoun-Levi JM, Sun Myint A, et al. Past, present, and future of radiotherapy for the benefit of patients. Nat Rev Clin Oncol 2013;10:52–60. - PubMed
-
- Bahn E, Bauer J, Harrabi S, et al. Late contrast enhancing brain lesions in proton-treated patients with low-grade glioma: Clinical evidence for increased periventricular sensitivity and variable RBE. Int J Radiat Oncol Biol Phys 2020;107:571–578. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
