

Bilateral shoulder septic arthritis due to suspected bacterial endocarditis: A case report
- PMID: 33640641
- PMCID: PMC7921498
- DOI: 10.1016/j.ijscr.2021.02.010
Bilateral shoulder septic arthritis due to suspected bacterial endocarditis: A case report
Abstract
Introduction: Septic arthritis is an orthopedic emergency that requires rapid diagnosis and treatment. It is typically caused by occult bacteremia which allows bacteria to seed the joint or local invasion of a soft tissue infection. Most cases of septic arthritis are caused by gram-positive bacteria, with the most common culprit being Staphylococcus Aureus. The reason septic arthritis is an orthopedic emergency is because of rapid destruction to cartilage. The mechanism of injury to cartilage is two-fold: bacterial enzymes are directly toxic to joint cartilage, and buildup of exudate can tamponade blood flow and cause anoxic injury. Typically, the knee is the most commonly involved joint. This is followed by the hip, ankle, elbow, wrist, and shoulder in descending order of occurrence. Polyarticular disease makes up a small percentage of these cases and if present, it is usually asymmetric and will involve at least one knee joint.
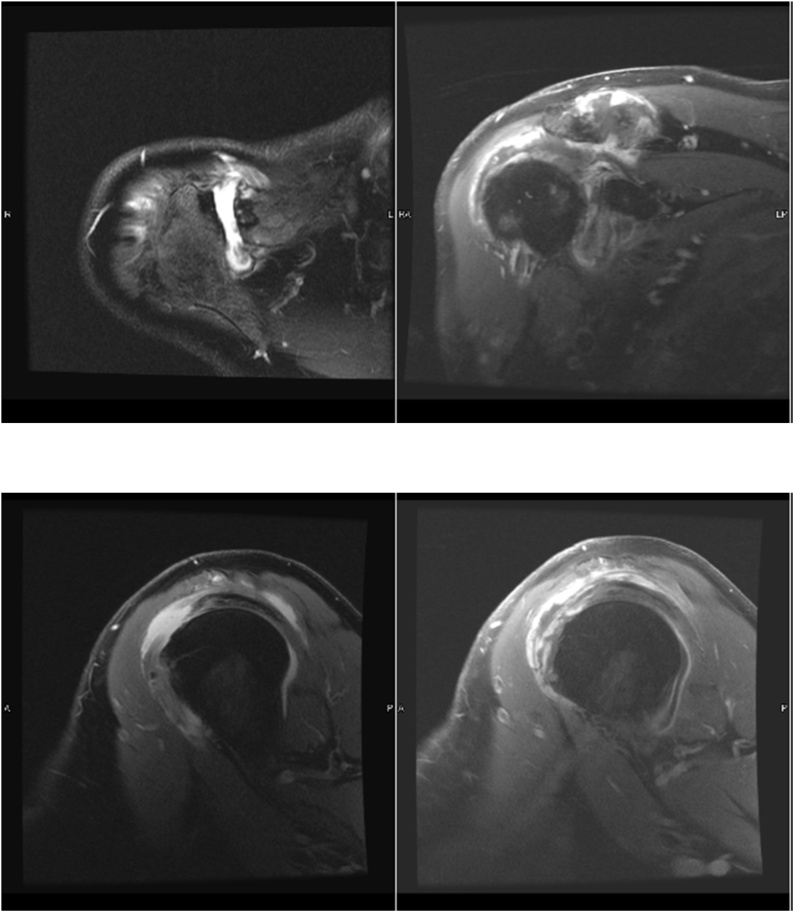
Presentation of case: Bilateral joint septic arthritis is relatively rare. We present an uncommon case of atraumatic bilateral septic shoulders in an elderly man with a history of heart disease and insidious bilateral shoulder pain after golfing 18 holes. This presentation is unique not only in its rarity but also in its impact on our understanding of septic arthritis in the setting of medical comorbidities and a relatively unimpressive presentation. With a recent golfing day just prior to presentation, differential diagnoses other than septic arthritis included deltoid/rotator cuff muscle strain, acute on chronic rotator cuff tendinosis, acute on chronic rotator cuff tearing, acute flare up of osteoarthritis, rheumatoid arthritis, or crystalline arthropathy. With elevated inflammatory markers and an equivocal physical examination, our patient underwent advanced imaging via MRI and subsequent bilateral glenohumeral joint diagnostic aspirations that were consistent with septic arthritis due to his complaining of contralateral shoulder pain shortly after his admission. Immediately after said diagnosis was made, the patient was taken back for emergent bilateral open irrigation and debridement, as septic arthritis is an orthopedic emergency, and went on to recover appropriately on culture-directed intravenous antibiotic therapy.
Discussion/conclusion: This case report is impactful with regard to clinical practice for multiple reasons. First and foremost it is a cautionary tale for all clinicians with regard to the level of suspicion one must have for polyarticular septic arthritis in the setting of the multiply painful patient. Second, it demonstrates the utility of advanced imaging in the equivocal patient. Lastly, it underscores the importance of prompt diagnosis and treatment, validating the existing algorithm for septic arthritis.
Keywords: Arthritis; Bilateral; Endocarditis; Infection; Septic; Shoulder.
Copyright © 2021 The Authors. Published by Elsevier Ltd.. All rights reserved.
Figures

Similar articles
-
Septic gonococcal arthritis in a pediatric patient: Rare case report.Int J Surg Case Rep. 2021 Mar;80:105701. doi: 10.1016/j.ijscr.2021.105701. Epub 2021 Feb 24. Int J Surg Case Rep. 2021. PMID: 33667910 Free PMC article.
-
Bilateral glenohumeral septic arthritis secondary to mastitis with subsequent avascular necrosis: A case report.Int J Surg Case Rep. 2021 Nov;88:106502. doi: 10.1016/j.ijscr.2021.106502. Epub 2021 Oct 15. Int J Surg Case Rep. 2021. PMID: 34666252 Free PMC article.
-
Erosive bilateral glenohumeral osteoarthritis caused by urosepsis-induced septic arthritis.JAAPA. 2024 Dec 1;37(12):25-28. doi: 10.1097/01.JAA.0000000000000139. Epub 2024 Dec 21. JAAPA. 2024. PMID: 39569854
-
Septic arthritis of the lumbar facet joint presenting as spontaneous bacterial peritonitis: a rare case requiring surgical intervention.Eur J Orthop Surg Traumatol. 2020 Jan;30(1):175-178. doi: 10.1007/s00590-019-02527-y. Epub 2019 Aug 29. Eur J Orthop Surg Traumatol. 2020. PMID: 31463672 Review.
-
[Differential therapy for the rheumatoid shoulder].Orthopade. 2002 Dec;31(12):1132-44. doi: 10.1007/s00132-002-0401-2. Orthopade. 2002. PMID: 12486539 Review. German.
Cited by
-
MRSA in the bursa: an unusual complication of MRSA bacteremia causing bilateral acromioclavicular septic arthritis.Access Microbiol. 2022 Dec 5;4(12):acmi000438. doi: 10.1099/acmi.0.000438. eCollection 2022. Access Microbiol. 2022. PMID: 36644736 Free PMC article.
References
-
- Goldenberg D.L., Sexton D.J. UpToDate; 1985. Septic Arthritis in Adults. p. 20.
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
