

Resource requirements for reintroducing elective surgery during the COVID-19 pandemic: modelling study
- PMID: 33640927
- PMCID: PMC7799203
- DOI: 10.1093/bjs/znaa012
Resource requirements for reintroducing elective surgery during the COVID-19 pandemic: modelling study
Abstract
Background: The COVID-19 response required the cancellation of all but the most urgent surgical procedures. The number of cancelled surgical procedures owing to Covid-19, and the reintroduction of surgical acivirt, was modelled.
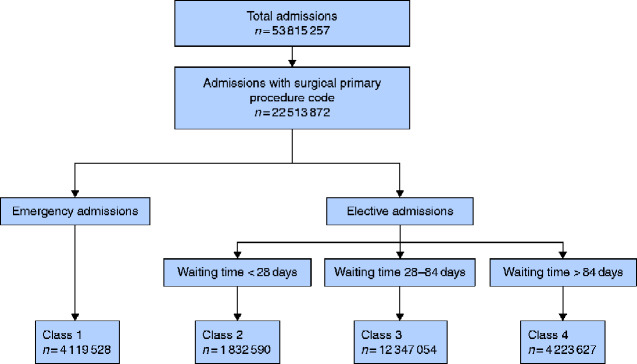
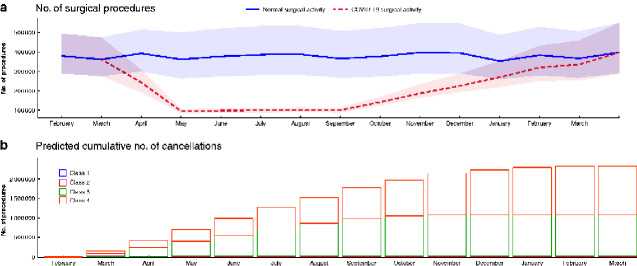
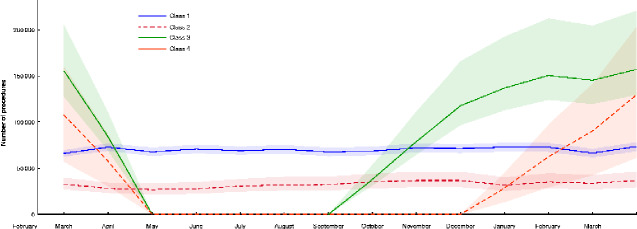
Methods: This was a modelling study using Hospital Episode Statistics data (2014-2019). Surgical procedures were grouped into four urgency classes. Expected numbers of surgical procedures performed between 1 March 2020 and 28 February 2021 were modelled. Procedure deficit was estimated using conservative assumptions and the gradual reintroduction of elective surgery from the 1 June 2020. Costs were calculated using NHS reference costs and are reported as millions or billions of euros. Estimates are reported with 95 per cent confidence intervals.
Results: A total of 4 547 534 (95 per cent c.i. 3 318 195 to 6 250 771) patients with a pooled mean age of 53.5 years were expected to undergo surgery between 1 March 2020 and 28 February 2021. By 31 May 2020, 749 247 (513 564 to 1 077 448) surgical procedures had been cancelled. Assuming that elective surgery is reintroduced gradually, 2 328 193 (1 483 834 - 3 450 043) patients will be awaiting surgery by 28 February 2021. The cost of delayed procedures is €5.3 (3.1 to 8.0) billion. Safe delivery of surgery during the pandemic will require substantial extra resources costing €526.8 (449.3 to 633.9) million.
Conclusion: As a consequence of the Covid-19 pandemic, provision of elective surgery will be delayed and associated with increased healthcare costs.
Antecedentes: La respuesta COVID-19 requirió la cancelación de todos los procedimientos quirúrgicos excepto los más urgentes. Se realizó un estudio de modelado del número de procedimientos quirúrgicos cancelados en el Servicio Nacional de Salud (National Health Service, NHS) de Inglaterra con motivo de la COVID-19 y de la reintroducción de la actividad quirúrgica.
Métodos: Estudio de modelado con datos de la Estadística de Episodios Hospitalarios (2014-2019). Utilizando las definiciones de NHS de Inglaterra, los procedimientos quirúrgicos se agruparon en cuatro clases de urgencias. Se modeló el número esperado de procedimientos quirúrgicos realizados entre el 1 de marzo de 2020 y el 28 de febrero de 2021. El déficit de procedimientos se estimó utilizando supuestos conservadores y una reintroducción gradual de la cirugía electiva a partir del 1 de junio de 2020. Los costes se calcularon utilizando los costes de referencia del NHS y se expresan en millones (M) o miles de millones (B) de euros (€). Las estimaciones se presentan con los i.c. del 95%.
Resultados: Se esperaba que 4.547.534 (3.318.195 – 6.250.771) pacientes con una edad media de 53,5 años se sometieran a cirugía entre el 1 de marzo de 2020 y el 28 de febrero de 2021. A fecha del 31 de mayo de 2020, 749.247 (513.564 – 1.077.448) intervenciones quirúrgicas habían sido canceladas. Suponiendo que la cirugía electiva se reintroduzca gradualmente, 2.328.193 (1.483.834 – 3.450.043) pacientes estarán en espera de cirugía antes del 28 de febrero de 2021. El coste de los procedimientos retrasados es de 5,3 mil millones de euros (3,1 mil millones - 8,0 mil millones de euros). La realización segura de una cirugía durante la pandemia requerirá recursos adicionales sustanciales que cuestan 526,8 millones de euros (449,6 millones de euros - 633,9 millones de euros).
Conclusión: La reintroducción de la cirugía electiva en el NHS de Inglaterra se asociará con retrasos sustanciales en el tratamiento y grandes aumentos de costes. Los desafíos y costes de reintroducir la atención quirúrgica en otros entornos asistenciales pueden ser distintos y se requiere con urgencia más estudios con el fin de monitorizar la recuperación de la atención quirúrgica.
The Author(s) 2020. Published by Oxford University Press on behalf of BJS Society Ltd. All rights reserved. For permissions, please email: journals.permissions@oup.com.
Figures
References
-
- Abbott TEF, Fowler AJ, Dobbs TD, Harrison EM, Gillies MA, Pearse RM. Frequency of surgical treatment and related hospital procedures in the UK: a national ecological study using hospital episode statistics. Br J Anaesth 2017;119:249–257 - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
