

Surgical outcomes after radioactive 125I seed versus hookwire localization of non-palpable breast cancer: a multicentre randomized clinical trial
- PMID: 33640932
- PMCID: PMC10364908
- DOI: 10.1093/bjs/znaa008
Surgical outcomes after radioactive 125I seed versus hookwire localization of non-palpable breast cancer: a multicentre randomized clinical trial
Abstract
Background: Previous studies have suggested improved efficiency and patient outcomes with 125I seed compared with hookwire localization (HWL) in breast-conserving surgery, but high-level evidence of superior surgical outcomes is lacking. The aim of this multicentre pragmatic RCT was to compare re-excision and positive margin rates after localization using 125I seed or hookwire in women with non-palpable breast cancer.
Methods: Between September 2013 and March 2018, women with non-palpable breast cancer eligible for breast-conserving surgery were assigned randomly to preoperative localization using 125I seeds or hookwires. Randomization was stratified by lesion type (pure ductal carcinoma in situ (DCIS) or other) and study site. Primary endpoints were rates of re-excision and margin positivity. Secondary endpoints were resection volumes and weights.
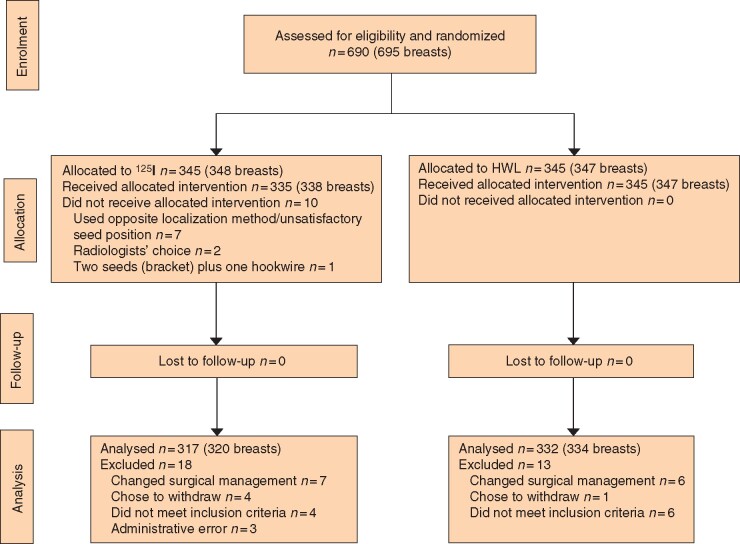
Results: A total of 690 women were randomized at eight sites; 659 women remained after withdrawal (125I seed, 327; HWL, 332). Mean age was 60.3 years in the 125I seed group and 60.7 years in the HWL group, with no difference between the groups in preoperative lesion size (mean 13.2 mm). Lesions were pure DCIS in 25.9 per cent. The most common radiological lesion types were masses (46.9 per cent) and calcifications (28.2 per cent). The localization modality was ultrasonography in 65.5 per cent and mammography in 33.7 per cent. The re-excision rate after 125I seed localization was significantly lower than for HWL (13.9 versus 18.9 per cent respectively; P = 0.019). There were no significant differences in positive margin rates, or in specimen weights and volumes.
Conclusion: Re-excision rates after breast-conserving surgery were significantly lower after 125I seed localization compared with HWL. Registration number: ACTRN12613000655741 (http://www.ANZCTR.org.au/).
© The Author(s) 2020. Published by Oxford University Press on behalf of BJS Society Ltd.
Figures
References
-
- Cady B, Stone MD, Schuler JG, Thakur R, Wanner MA, Lavin PT. The new era in breast cancer: invasion, size, and nodal involvement dramatically decreasing as a result of mammographic screening. Arch Surg 1996;131:301–308 - PubMed
-
- Chadwick D, Shorthouse A. Wire-directed localization biopsy of the breast: an audit of results and analysis of factors influencing therapeutic value in the treatment of breast cancer. Eur J Surg Oncol 1997;23:128–133 - PubMed
-
- Ballal H, Taylor DB, Bourke AG, Latham B, Saunders CM. Predictors of re-excision in wire-guided wide local excision for early breast cancer: a Western Australian multi-centre experience. ANZ J Surg 2015;85:540–545 - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
