

Efficacy and Safety of Intravenous rtPA in Ischemic Strokes Due to Small-Vessel Occlusion: Systematic Review and Meta-Analysis
- PMID: 33641037
- PMCID: PMC8055574
- DOI: 10.1007/s12975-021-00890-9
Efficacy and Safety of Intravenous rtPA in Ischemic Strokes Due to Small-Vessel Occlusion: Systematic Review and Meta-Analysis
Abstract
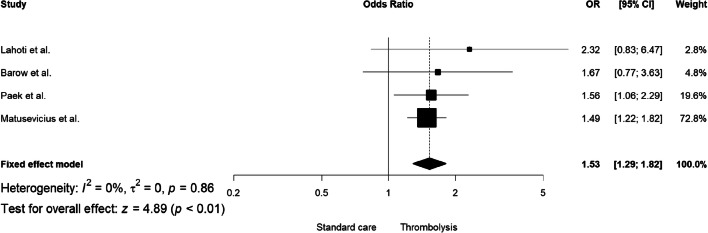
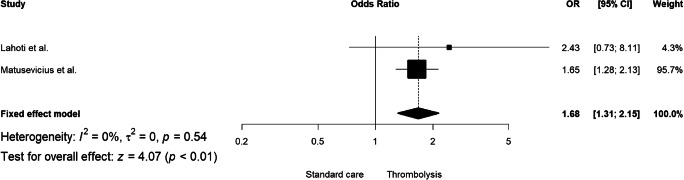
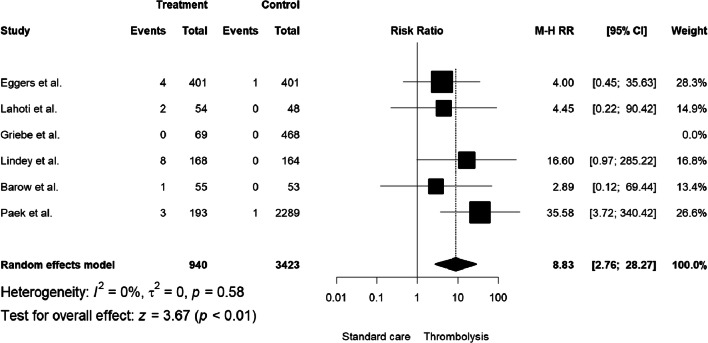
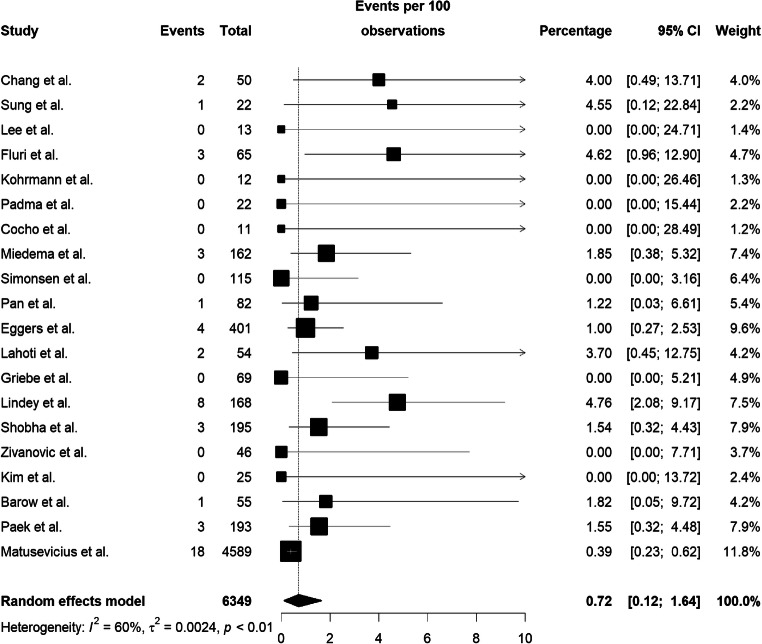
Intravenous recombinant tissue plasminogen activator (iv-rtPA) has been routinely used to treat ischemic stroke for 25 years, following large clinical trials. However, there are few prospective studies on the efficacy and safety of this therapy in strokes attributed to cerebral small vessel disease (SVD). We evaluated functional outcome (modified Rankin scale, mRS) and symptomatic intracerebral hemorrhage (sICH) using all available data on the effects of iv-rtPA in SVD-related ischemic stroke (defined either using neuroimaging, clinical features, or both). Using fixed-effect and random-effects models, we calculated the pooled effect estimates with regard to excellent and favorable outcomes (mRS=0-1 and 0-2 respectively, at 3 months), and the rate of sICH. Twenty-three studies fulfilled the eligibility criteria, 11 of which were comparative, and there were only 3 randomized clinical trials. In adjusted analyses, there was an increased odds of excellent outcome (adjusted OR=1.53, 95% CI: 1.29-1.82, I2: 0%) or favorable outcome (adjusted OR=1.68, 95% CI: 1.31-2.15,I2: 0%) in patients who received iv-rtPA compared with placebo. Across the six studies which reported it, the incidence of sICH was higher in the treatment group (M-H RR = 8.83, 95% CI: 2.76-28.27). The pooled rate of sICH in patients with SVD administered iv-rtPA was only 0.72% (95% CI: 0.12%-1.64%). We conclude that when ischemic stroke attributed to SVD is considered separately, available data on the effects of iv-rtPA therapy are insufficient for the highest level of recommendation, but it seems to be safe. Although further therapeutic trials in SVD-related ischemic stroke appear to be justified, our findings should not prevent its continued use for this group of patients in clinical practice.
Keywords: Brain ischemia; Lacunar infarction; Meta-analysis; Small vessel disease; Stroke; Thrombolysis.
Conflict of interest statement
BK received salaries for providing lectures at the Boehringer Ingelheim sponsored symposia within larger scientific or clinical conferences. All information provided by BK during his lectures is solely and exclusively based on systematic evidence-based knowledge on the subject, and do not contain any commercial promotional data. DJW has received personal fees from Bayer, Alnylam and Portola.
Figures
References
-
- Hacke W, Kaste M, Cesare F, Toni D, Lesaffre E, von Kummer R, et al. Intravenous thrombolysis with recombinant tissue plasminogen activator for acute hemispheric stroke. JAMA. 1995;274:1017–1025. - PubMed
-
- Hacke W, Kaste M, Fieschi C, von Kummer R, Davalos A, Meier D, Larrue V, Bluhmki E, Davis S, Donnan G, Schneider D, Diez-Tejedor E, Trouillas P. Randomised double-blind placebo-controlled trial of thrombolytic therapy with intravenous alteplase in acute ischaemic stroke (ECASS II) Lancet. 1998;352:1245–1251. - PubMed
-
- Hacke W, Kaste M, Bluhmki E, Brozman M, Dávalos A, Guidetti D, et al. Thrombolysis with Alteplase 3 to 4.5 hours after acute ischemic stroke Werner. N Engl J Med. 2008;359:1543–1554. - PubMed
-
- Sandercock P, Wardlaw JM, Lindley RI, Dennis M, Cohen G, Murray G, et al. The benefits and harms of intravenous thrombolysis with recombinant tissue plasminogen activator within 6 h of acute ischaemic stroke (the third international stroke trial [IST-3]): a randomised controlled trial. Lancet. 2012;379:2352–2363. - PMC - PubMed
-
- Clark WM, Wissman S, Albers GW, Jhamandas JH, Madden KP, Hamilton S, et al. Recombinant tissue-type plasminogen activator (Alteplase) for ischemic stroke 3 to 5 hours after symptom onset. JAMA. 2003;282:2019–2026. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical