

Lymphatic pathway evaluation in congenital heart disease using 3D whole-heart balanced steady state free precession and T2-weighted cardiovascular magnetic resonance
- PMID: 33641664
- PMCID: PMC7919323
- DOI: 10.1186/s12968-021-00707-6
Lymphatic pathway evaluation in congenital heart disease using 3D whole-heart balanced steady state free precession and T2-weighted cardiovascular magnetic resonance
Abstract
Background: Due to passive blood flow in palliated single ventricle, central venous pressure increases chronically, ultimately impeding lymphatic drainage. Early visualization and treatment of these malformations is essential to reduce morbidity and mortality. Cardiovascular magnetic resonance (CMR) T2-weighted lymphangiography (T2w) is used for lymphatic assessment, but its low signal-to-noise ratio may result in incomplete visualization of thoracic duct pathway. 3D-balanced steady state free precession (3D-bSSFP) is commonly used to assess congenital cardiac disease anatomy. Here, we aimed to improve diagnostic imaging of thoracic duct pathway using 3D-bSSFP.
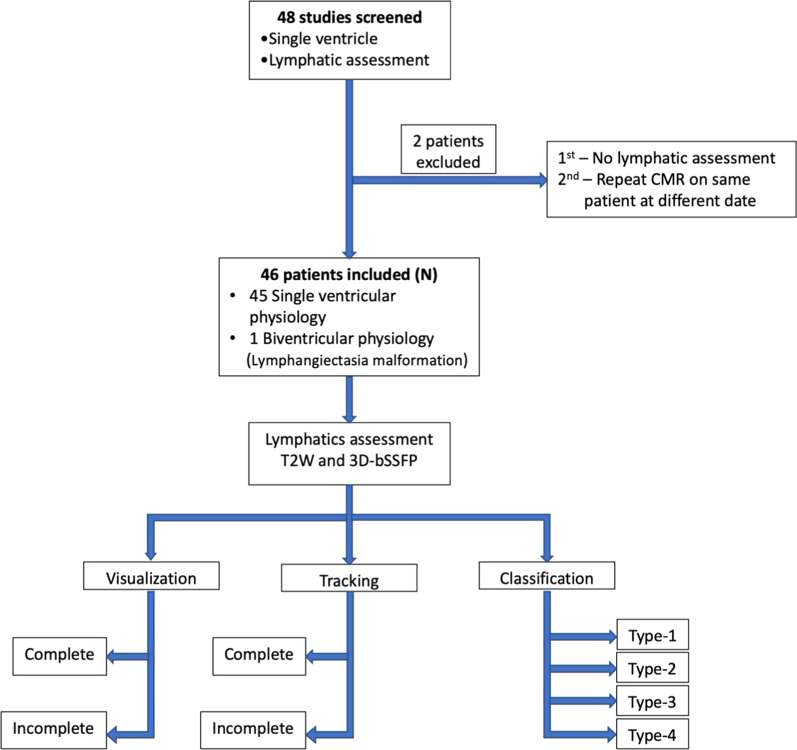
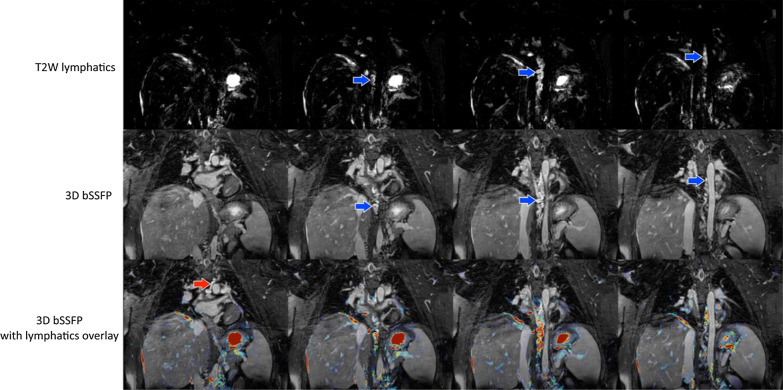
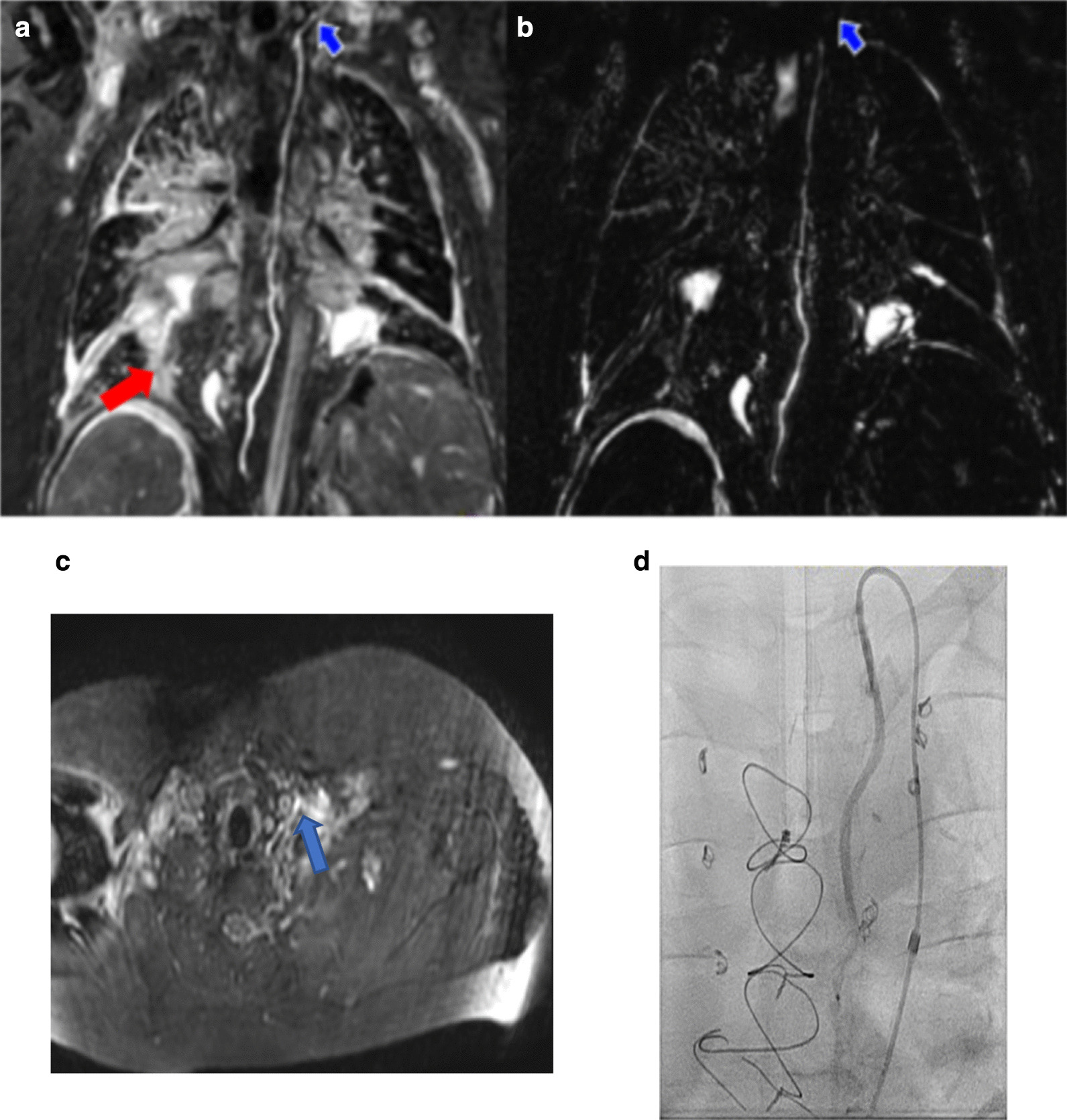
Methods: Patients underwent CMR during single ventricle or central lymphatic system assessment using T2w and 3D-bSSFP. T2w parameters included 3D-turbo spin echo (TSE), TE/TR = 600/2500 ms, resolution = 1 × 1 × 1.8 mm, respiratory triggering with bellows. 3D-bSSFP parameters included electrocardiogram triggering and diaphragm navigator, 1.6 mm isotropic resolution, TE/TR = 1.8/3.6 ms. Thoracic duct was identified independently in T2w and 3D-bSSFP images, tracked completely from cisterna chyli to its drainage site, and classified based on severity of lymphatic abnormalities.
Results: Forty-eight patients underwent CMR, 46 of whom were included in the study. Forty-five had congenital heart disease with single ventricle physiology. Median age at CMR was 4.3 year (range 0.9-35.1 year, IQR 2.4 year), and median weight was 14.4 kg (range, 7.9-112.9 kg, IQR 5.2 kg). Single ventricle with right dominant ventricle was noted in 31 patients. Thirty-eight patients (84%) were status post bidirectional Glenn and 7 (16%) were status post Fontan anastomosis. Thoracic duct visualization was achieved in 45 patients by T2w and 3D-bSSFP. Complete tracking to drainage site was attained in 11 patients (24%) by T2w vs 25 (54%) by 3D-bSSFP and in 28 (61%) by both. Classification of lymphatics was performed in 31 patients.
Conclusion: Thoracic duct pathway can be visualized by 3D-bSSFP combined with T2w lymphangiography. Cardiac triggering and respiratory navigation likely help retain lymphatic signal in the retrocardiac area by 3D-bSSFP. Visualizing lymphatic system leaks is challenging on 3D-bSSFP images alone, but 3D-bSSFP offers good visualization of duct anatomy and landmark structures to help plan interventions. Together, these sequences can define abnormal lymphatic pathway following single ventricle palliative surgery, thus guiding lymphatic interventional procedures.
Keywords: 3D-balanced SSFP; Cardiac catheterization; Congenital heart disease; Interventional CMR; Lymphatic imaging; Lymphatic intervention; Magnetic resonance imaging; SSFP; Single ventricle; T2-weighted imaging.
Conflict of interest statement
The author(s) declare that they have no competing interests.
Figures

References
-
- Atz AM, Zak V, Mahony L, Uzark K, Shrader P, Gallagher D, Paridon SM, Williams RV, Breitbart RE, Colan SD, et al. Survival data and predictors of functional outcome an average of 15 years after the Fontan procedure: the pediatric heart network Fontan cohort. Congenit Heart Dis. 2015;10(1):E30–42. doi: 10.1111/chd.12193. - DOI - PMC - PubMed
-
- Brace RA, Valenzuela GJ. Effects of outflow pressure and vascular volume loading on thoracic duct lymph flow in adult sheep. Am J Physiol. 1990;258(1 Pt 2):R240–244. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
