

Cardiotoxicity Induced by Immune Checkpoint Inhibitors: A Pharmacovigilance Study From 2014 to 2019 Based on FAERS
- PMID: 33643048
- PMCID: PMC7907652
- DOI: 10.3389/fphar.2021.616505
Cardiotoxicity Induced by Immune Checkpoint Inhibitors: A Pharmacovigilance Study From 2014 to 2019 Based on FAERS
Abstract
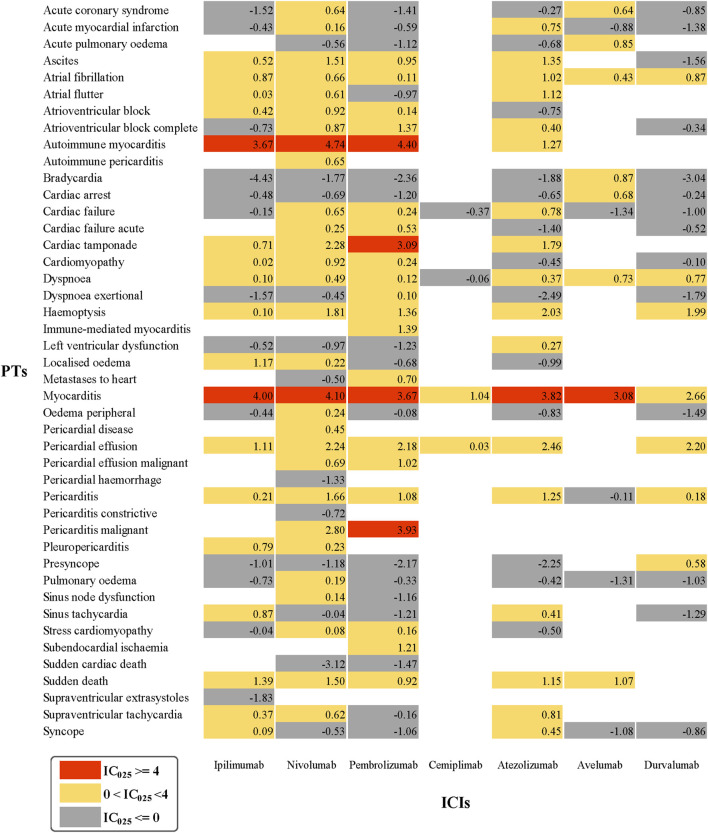
This study was to scientifically and systematically explore the association between cardiotoxicity and immune checkpoint inhibitors (ICIs) and also to characterize the spectrum of ICI-related cardiac complications. From the first quarter of 2014 to the fourth quarter of 2019, data from the FDA Adverse Event Reporting System database were selected to conduct the disproportionality analysis. Reporting odds ratios and information components were used to evaluate the signal after statistical shrinkage transformation. In total, 7,443,137 cases and 36,326,611 drug-adverse event pairs were collected, among which 9,271 cases were identified to be related to ICI-induced cardiotoxicities. The number of male patients was much higher than that of females (5,579 vs. 3,031) and males presented a slightly higher reporting frequency than females in general, which was statistically significant (ROR = 1.04, 95%CI: 0.99-1.09, p < 0.001). Simultaneously, the proportion of serious or life-threatening outcomes in males was significantly higher than in females (ROR = 1.05, 95%CI: 0.96-1.15, p < 0.001). Importantly, ICIs were associated with over-reporting frequencies of cardiotoxicities in general (ROR025 = 1.06, IC025 = 0.08). PD-1 and PD-L1 were found to be related to cardiac adverse events, corresponding to ROR025 = 1.06, IC025 = 0.08, and ROR025 = 1.06, IC025 = 0.08, respectively, while anti-CTLA-4 (cytotoxic T-lymphocyte-associated protein 4) was significantly associated with some specific adverse events rather than common adverse events. The spectrum of cardiotoxicities induced by ICIs mostly differed among individual agents, but also demonstrated some common features. Dyspnea (N = 2,527, 21.25%), myocarditis (N = 614, 5.16%), atrial fibrillation (N = 576, 4.84%), cardiac failure (N = 476, 4.00%), and pericardial effusion (N = 423, 3.56%) were the top five cardiac adverse events reported in the database. Among them, myocarditis was the only one caused by all ICIs with strong signal value and high risk, warranting further attention. Overall, this investigation mainly showed the profile of cardiotoxicities caused by ICIs, which varied between different ICI therapies, but also shared some similarities in specific symptoms such as myocarditis. Therefore, it is vital and urgent to recognize and manage ICI-related cardiotoxicities, known to frequently occur in clinical practice, at the earliest point.
Keywords: FAERS; adverse drug reaction; cardiotoxicity; disproportionality analysis; immune checkpoint inhibitors; information component; pharmacovigilance; reporting odds ratio.
Copyright © 2021 Chen, Chen, Liang, Guo, Xu, Zheng, Guo, Chi, Wei, Chen, Ye and He.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Endocrine toxicity of immune checkpoint inhibitors: a real-world study leveraging US Food and Drug Administration adverse events reporting system.J Immunother Cancer. 2019 Nov 6;7(1):286. doi: 10.1186/s40425-019-0754-2. J Immunother Cancer. 2019. PMID: 31694698 Free PMC article.
-
Cardiac arrhythmias associated with immune checkpoint inhibitors: A comprehensive disproportionality analysis of the FDA adverse event reporting system.Front Pharmacol. 2022 Nov 4;13:986357. doi: 10.3389/fphar.2022.986357. eCollection 2022. Front Pharmacol. 2022. PMID: 36408225 Free PMC article.
-
Pancreatic Adverse Events Associated With Immune Checkpoint Inhibitors: A Large-Scale Pharmacovigilance Analysis.Front Pharmacol. 2022 Apr 1;13:817662. doi: 10.3389/fphar.2022.817662. eCollection 2022. Front Pharmacol. 2022. PMID: 35431928 Free PMC article.
-
PD-1/PD-L1 inhibitor-induced immune thrombocytopenia: A pharmacovigilance study and systematic review.Int Immunopharmacol. 2024 Mar 10;129:111606. doi: 10.1016/j.intimp.2024.111606. Epub 2024 Feb 14. Int Immunopharmacol. 2024. PMID: 38359661
-
Acute kidney injury associated with immune checkpoint inhibitors: A pharmacovigilance study.Int Immunopharmacol. 2022 Dec;113(Pt A):109350. doi: 10.1016/j.intimp.2022.109350. Epub 2022 Oct 20. Int Immunopharmacol. 2022. PMID: 36272360
Cited by
-
Safety of Glucagon-Like Peptide-1 Receptor Agonists: A Real-World Study Based on the US FDA Adverse Event Reporting System Database.Clin Drug Investig. 2022 Nov;42(11):965-975. doi: 10.1007/s40261-022-01202-1. Epub 2022 Sep 30. Clin Drug Investig. 2022. PMID: 36175609
-
Cardiomyopathies and a brief insight into DOX-induced cardiomyopathy.Egypt Heart J. 2025 Mar 10;77(1):29. doi: 10.1186/s43044-025-00628-0. Egypt Heart J. 2025. PMID: 40064787 Free PMC article. Review.
-
Adverse Events During Pregnancy Associated With Entecavir and Adefovir: New Insights From a Real-World Analysis of Cases Reported to FDA Adverse Event Reporting System.Front Pharmacol. 2022 Jan 3;12:772768. doi: 10.3389/fphar.2021.772768. eCollection 2021. Front Pharmacol. 2022. PMID: 35046808 Free PMC article.
-
Differences in hypersensitivity reactions and gadolinium deposition disease/symptoms associated with gadolinium exposure to gadolinium-based contrast agents: new insights based on global databases VigiBase, FAERS, and IQVIA-MIDAS.BMC Med. 2024 Aug 13;22(1):329. doi: 10.1186/s12916-024-03537-2. BMC Med. 2024. PMID: 39135199 Free PMC article.
-
Immune checkpoint inhibitors and cardiovascular toxicity: immunology, pathophysiology, diagnosis, and management.J Thromb Thrombolysis. 2025 Jul 17. doi: 10.1007/s11239-025-03146-7. Online ahead of print. J Thromb Thrombolysis. 2025. PMID: 40673965 Review.
References
-
- Barlesi F., Vansteenkiste J., Spigel D., Ishii H., Garassino M., de Marinis F., et al. (2018). Avelumab versus docetaxel in patients with platinum-treated advanced non-small-cell lung cancer (JAVELIN Lung 200): an open-label, randomised, phase 3 study. The Lancet Oncol. 19 (11), 1468–1479. 10.1016/S1470-2045(18)30673-9 - DOI - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials